Filling in the holes of recent stories in the New York Times, and Propublica on the outpatient care of patients with peripheral arterial disease
Most have gotten used to egregiously bad coverage of current events that fills the pages of today’s New York Times, but even by their now very low standards a recent telling of a story about peripheral artery disease was very bad.
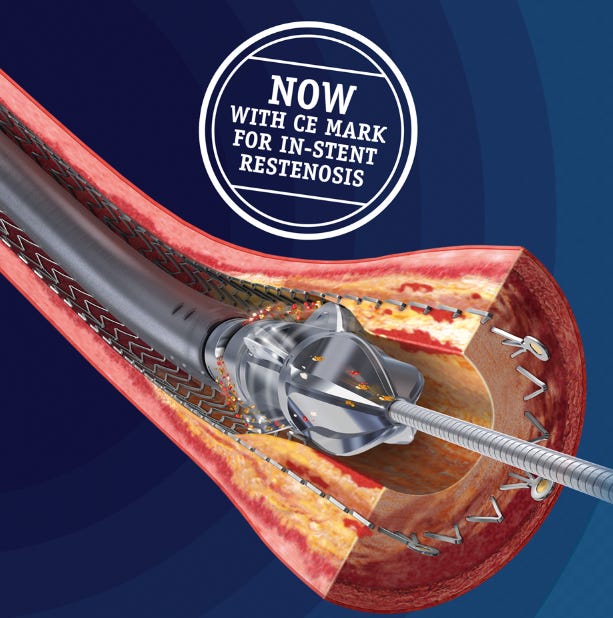
The scintillating allegation by Katie Thomas, Jessica Silver-Greenberg and Robert Gebeloff is that “medical device makers are bankrolling doctors to perform artery clearing procedures that can lead to amputations”.
The reporters go on to tell a story about patient Kelly Hanna, who presented to a physician, Dr. Jihad Mustapha, in a private clinic with a festering wound. After being diagnosed with a poor flow to her leg that was likely contributing to the wound, Dr. Mustapha performed multiple procedures on her leg to improve blood flow in an attempt to ward off a future amputation. The procedures were unsuccessful, and Ms. Hanna ultimately did need an amputation.
The All-in podcast is a fairly popular show that features successful silicon valley investors commenting about everything worth commenting on from politics to health. The group has good chemistry and interesting insights that breaks the mold of the usual tribal politics that controls legacy media analysis of current events.
Brad Gerstner, who is actually a guest host for this particular episode starts off by referencing something called Heartflow to evaluate the heart that has been recommended by one of the other hosts: Chamath Palihapitiya. Brad apparently asked his primary care physician about Heartflow and was instead directed to get a calcium scan.
Heartflow is a proprietary technology that purports to evaluate the presence of significant narrowing in the coronary arteries just by doing a heart CT scan. A calcium score is a low-dose CT scan used to identify the presence of calcium in coronary vessels.
The segment ends with a recommendation for everyone over the age of 40 to get some type of heart scan, so I thought it would be worth reviewing some of the main claims.
Question 1. Does Brad need a calcium scan?
Brad notes that his primary care physician told him he was young, fit, and had a low bad cholesterol (LDL) and needed a calcium scan rather than a heart flow scan. The answer to this question and the questions to follow depend on what outcome Brad is looking for. If the goal is to feel happier knowing if he has coronary calcium than the resounding answer is to get the calcium scan. But if the goal is to live longer and healthier, there is nothing to suggest a calcium scan will help. Most cardiologists believe that the lower the LDL, the better cardiovascular outcomes are. So if a calcium scan convinces Brad to NOT lower his LDL further either naturally or with medications, a calcium scan may be detrimental.
We have zero evidence to suggest patients who get calcium scans lower their risk of future mortality.
A national study from Korea published in the European Heart Journal sheds important new light on complications related to COVID vaccine related myocarditis. While US public health authorities have been convinced from the very beginning about how safe and effective the new vaccines are, researchers in other countries with far smaller budgets have been testing that theory.
It was Israeli researchers that first highlighted the novel mRNA vaccines as potentially causing myocarditis in the Spring of 2021, but it has proven difficult to quantify the risk of severe complications beyond scattered case reports of severe morbidity and mortality. In part, US researchers are hampered by vaccine reporting systems in the US that are passive surveillance systems relying on voluntary reporting of vaccine adverse events. This has the potential of under-reporting adverse events, which was exactly the conclusion of an earlier JAMA analysis on US VAERS vaccine myocarditis cases.
Diving deep into the methods and results of the study
The South Korean approach was to organize a national reporting system under the auspices of the Korean Disease Control and Prevention Agency (KDCA). The KDCA also established a reporting system with a legal obligation for special adverse events including myocarditis and pericarditis after COVID-19 vaccination. To evaluate all reported cases of suspected myocarditis or pericarditis after COVID-19 vaccination, the KDCA organized an “Expert Adjudication Committee on COVID-19 Vaccination Pericarditis/Myocarditis”. The committee comprised 7 experts in cardiology, 1 in infectious disease, 2 in epidemiology, epidemiologic investigators in 16 regional centers, and officials from the KDCA.
Among 44,276,704 subjects vaccinated from 26 February to 31 December 2021, 1533 cases of suspected myocarditis were reported to the KDCA. The committee adopted the myocarditis case definition and classification of the Brighton Collaboration (BC) (see figure below) for the diagnosis and degree of certainty of a Vaccine Related Myocarditis (VRM) diagnosis.
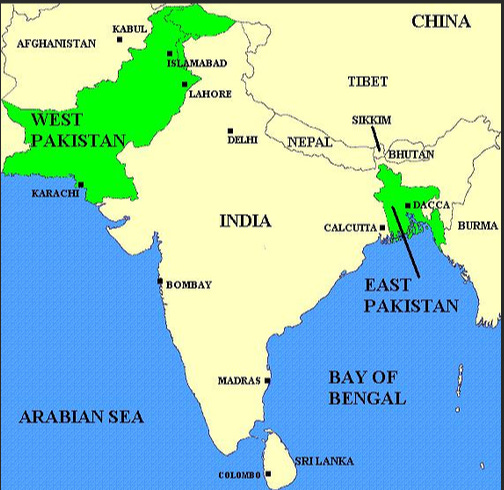
On March 25th, 1971, the Pakistani army launched Operation Searchlight, a military campaign to brutally suppress a Bengali nationalist movement.
The roots of the genocide lie in the parting gift British rulers gave to the Indian subcontinent at the time of independence in 1947. British controlled India was separated into Hindu majority India and Muslim majority Pakistan. But because there were two dense non-contiguous Muslim majority areas in British controlled India, the muslim majority country of Pakistan was divided into East and West Pakistan.
East and West Pakistan were linked by religion, but little else. East Pakistan was culturally Bengali, and had much more in common with Bengali Hindus than Muslims in West Pakistan. While Bengalis took pride in their culture and language, West Pakistani’s looked down on the Bengali’s because it was deemed to be too influenced by Hindu culture. While Bengali muslims may have identified themselves with Pakistan’s islamic project, by the 1970s many in East Pakistan had given priority to their Bengali ethnicity over their religious identity, desiring a society more in accordance with Western principles of secularism and democracy. A growing opposition in East Pakistan strongly objected to the Islamist paradigm being imposed the West Pakistani state.
But West Pakistan controlled the military, and formed much of the ruling elite after the partition in 1947. In a move designed to send a message to Bengali speaking East Pakistani’s , the founding father of Pakistan, Muhammad Jinna even made Urdu the national language of all of Pakistan, and branded those opposed as enemies of the State.
If there was any doubt the academic research enterprise is completely broken, we have an absolute train wreck of a study in one of the many specialty journals of the Journal of the American Medical Association — JAMA Health.
I had no idea the journal even existed until today, but I now know to approach the words printed in this journal to the words printed in supermarket tabloids. You should too!
The paper that was brought to my attention is one that purports to examine the deleterious health effects of Long COVID. A sizable group of intellectuals who are still socially distancing and wearing n95s live in fear of a syndrome that persists long after a person recovers from COVID. There are any number of papers that argue a variety of putative mechanisms for how an acute COVID infection may result in long term health concerns. This particular piece of research that is amplified by the usual credentialed suspects on social media found “increased rates of adverse outcomes over a 1-year period for a PCC (post-COVID conditions) cohort surviving the acute phase of illness.”
In this case PCC (Post-COVID conditions), is the stand-in for Long COVID, and leading commentators use this paper to explicitly state that heart attacks, strokes and other major adverse outcomes doubled in people post-COVID at 1 year…
It is a crazy statement, and anyone regurgitating this has no business commenting on any scientific papers. Let me explain why.
In order to find out about the potential ravages of long COVID researchers need to be able to compare outcomes between those who were infected with COVID and now have long covid to those who were never infected with COVID. At this point finding a large enough group of people that never had covid is impossible, because everyone in the world will have been infected with COVID many, many times. It’s also really hard to define the nebulous long COVID because a study after study finds no clear objective markers of the disease.
The COVID19/vaccine myocarditis debate continues in large part because our public health institutions are grossly mischaracterizing the risks and benefits of vaccines to young people.
A snapshot of what the establishment says as it relates to the particular area of concern: college vaccine mandates:
Dr. Arthur Reingold, an epidemiology professor at UC-Berkeley, notes that UC also requires immunizations for measles and chickenpox, and people still are dying from COVID at rates that exceed those for influenza. As of Feb. 1, there were more than 400 COVID deaths a day across the U.S.
“The argument in favor of mandatory vaccination for COVID is no different than the argument for mandatory vaccination for flu, measles and meningitis,” Reingold said. “For a 20-year-old college student, how likely are they to die? The risk is very low. But it’s not zero. The vaccines are safe, so the argument of continuing to mandate vaccination fits very well with the argument for the other vaccines we continue to require.”
Safety is a relative term that needs to be constantly updated when you’re talking about administering a therapeutic to “not-yet-sick” individuals. We do not vaccinate against smallpox anymore because the absence of circulating smallpox (thanks to the smallpox vaccine campaign) makes the risks of the smallpoxt vaccine too great to be administered to the public.
We can argue endlessly about what exactly the risk of COVID19 was in the Spring of 2020, or 2021, but there should be little argument in 2023 that the risks of COVID pneumonia striking down a young healthy individual is now extremely low.
I recently saw a young man who came to see me because his place of future employment, a large health system was requiring him to complete the 1º series of his COVID-19 vaccination. He was concerned because he had chest pain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. He attempted to get a Johnson and Johnson vaccine and was told by pharmacists he was not allowed to mix and match this particular vaccine as he had already received an mRNA dose. With no other option, he came to ask me whether I thought a vaccine exemption was reasonable in his case. He already had a family medicine physician sign an exemption that had been denied by his future employer’s vaccine exemption committee. The young man works on the “back end” of the health system remotely from home and he has no patient contact. The entire process has caused him to lose his health insurance from his former employer, and he was now paying out of pocket for an expensive COBRA health insurance plan. What follows is my letter to the vaccine exemption review committee regarding his case. (Published with permission, only the relevant names have been changed/redacted)
Dear Vaccine Exemption Review Committee,
I am writing this letter on behalf of John Smith DOB: xx/xx/xx in regard to a mandate from xxxx Health that Mr. Smith receive a second dose of an mRNA vaccine to complete his primary COVID-19 vaccine series.
Mr. Smith has asked me to render an opinion specifically related to his cardiac risk of receiving a second dose of an mRNA vaccine. I am a board-certified cardiologist in Philadelphia, Pennsylvania, and have been in active clinical practice for 13 years.
After reviewing the details of his case, I have grave concerns about compelling him to receive a second dose of an mRNA vaccine and would like to outline the reasons for my conclusion in this letter. I am going to specifically discuss his risk of an important, now well-recognized, adverse event: vaccine myocarditis.
What follows is some important background information about vaccine myocarditis that has been gleaned over the last 2 years before I discuss the particulars of Mr. Smith’s case.
It is relevant to note here that as a physician active clinically in both the inpatient and outpatient arenas, I am an eyewitness to the severe toll COVID-19 took on my patients in the Spring or 2020. I was impressed enough with the initial mRNA vaccine data to acquire the vaccine available from the Philadelphia Department of Health (Moderna) and ran multiple vaccine clinics in order to vaccinate my mostly high-risk patients.
What follows is data produced since the vaccine rollout that is relevant to Mr. Smith’s case.
One of the hallmarks of the last two years has been the distance that frequently exists between published research and reality. I’m a cardiologist, and the first disconnect that became glaringly obvious very quickly was the impact COVID was having on the heart. As I walked through COVID rooms in the Spring of 2020 trying to hold my breath, I waited for a COVID cardiac tsunami. After all social media had been full of videos from Wuhan and Iran of people suddenly dropping in the streets. My hyperventilating colleagues made me hyperventilate. Could it be that Sars-COV2 had some predilection for heart damage?
Happily, I was destined for disappointment. There never was a cardiac tsunami from COVID.
There were, unhappily, lots of severely ill patients with lungs that were whited out who quickly developed multi-organ dysfunction while hospitalized. The lungs were where almost all the action was. Every other organ got hit hard because of the systemic illness that unfortunately often is a downstream result of a severe respiratory illness. Cardiac Cath labs waiting for some major influx of COVID heart damage not only didn’t see patients presenting with COVID heart attacks, but they idled as patients terrified of coming to the hospital stayed home rather than come to the hospital with chest pain. (Public health messaging about COVID appears to have kept people away from hospitals, and autopsy series of deaths during the pandemic found that reduced access to health care systems (for conditions such as myocardial infarction) was further likely to be identified as a contributory factor to death than undiagnosed COVID-19).
So imagine my surprise when I saw peer-reviewed research based on a cardiac MRI study come out in 2020 suggesting that 78% of patients who survived COVID may have significant heart damage. A more detailed read of the paper, of course, threw up massive problems. The article and authors were more suited as writers for Oprah and Dr. Phil than for a well-respected academic journal. But the damage was done, and the notion that COVID was attacking hearts spread via a social media influencer class that should have had the credentials and smarts to know better, but clearly didn’t.
Myopericarditis is a now a well reported complication associated with Sars-Cov-2 (COVID-19) vaccinations. This has been particularly common with the messenger RNA (mRNA) vaccines (BNT162b2 and mrna-1273), with a particular predilection for young males.
A just published report of 2 cases from Australia that document myopericarditis after use of the non-mRNA Novavax vaccine in patients that had recovered from mRNA vaccine myocarditis suggests this is a very bad idea.
The case reports
Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine. The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chest pain. The symptoms lasted 3 months, and a total of 6 months after the first episode of pericarditis, he received a booster vaccination with the Novovax (NVX-CoV2373) vaccine. 2-3 days after this he developed the same sharp chest pain and shortness of breath with elevated inflammatory markers (CRP) as well as typical findings of pericarditis seen on ECG. To add insult to injury, he contracted COVID 2 months after the second episode of pericarditis, but had no recurrence of the symptoms of pericarditis.
Reanalysis of a trial used to approve a commonly used injectable cholesterol-lowering drug confirms the original analysis by accident.
The open-data movement seeks to liberate the massive amount of data generated in running clinical trials from the grasp of the academic medical-pharmaceutical industrial complex that mostly runs the most important trials responsible for bringing novel therapeutics to market.
There are only a few elite academic trialist groups capable of running large trials and there’s ample reason to be suspicious about the nexus that has developed between academia and the pharmaceutical companies that shower them with cash to hopefully get a positive study result and pay off the pharmaceutical research investment manifold. The FDA is the major regulator of the whole process, but the expertise required for regulation means that the FDA is frequently comprised of ex-pharma employees or ex-academics.