
BY ANISH KOKA
The COVID19/vaccine myocarditis debate continues in large part because our public health institutions are grossly mischaracterizing the risks and benefits of vaccines to young people.
A snapshot of what the establishment says as it relates to the particular area of concern: college vaccine mandates:

Dr. Arthur Reingold, an epidemiology professor at UC-Berkeley, notes that UC also requires immunizations for measles and chickenpox, and people still are dying from COVID at rates that exceed those for influenza. As of Feb. 1, there were more than 400 COVID deaths a day across the U.S.
“The argument in favor of mandatory vaccination for COVID is no different than the argument for mandatory vaccination for flu, measles and meningitis,” Reingold said. “For a 20-year-old college student, how likely are they to die? The risk is very low. But it’s not zero. The vaccines are safe, so the argument of continuing to mandate vaccination fits very well with the argument for the other vaccines we continue to require.”
Safety is a relative term that needs to be constantly updated when you’re talking about administering a therapeutic to “not-yet-sick” individuals. We do not vaccinate against smallpox anymore because the absence of circulating smallpox (thanks to the smallpox vaccine campaign) makes the risks of the smallpoxt vaccine too great to be administered to the public.
We can argue endlessly about what exactly the risk of COVID19 was in the Spring of 2020, or 2021, but there should be little argument in 2023 that the risks of COVID pneumonia striking down a young healthy individual is now extremely low.
The other argument made by public health authorities is that myocarditis, the major adverse event linked to the mrna vaccines (Moderna worse than Pfizer), and Novovax actually happens more commonly with a COVID infection. I have made the case repeatedly since the Fall of 2020 that sars-cov2 (the virus that causes COVID), like the coronavirus family it comes from, has no specific proclivity for the heart, and that the published papers describing COVID19 myocarditis come from highly motivated cardiac imagers finding random bright spots on cardiac MRI devoid of clinical context and epidemiologists striking fools gold in research based on diagnostically sloppy electronic health record billing codes.
More evidence this past week that vaccine myocarditis is very much a real entity while COVID19 myocarditis is mostly a fabrication of academic researchers comes from Scandinavian countries.
A record request from a random Swedish twitter account reveals this impressive chart about myocarditis trends.
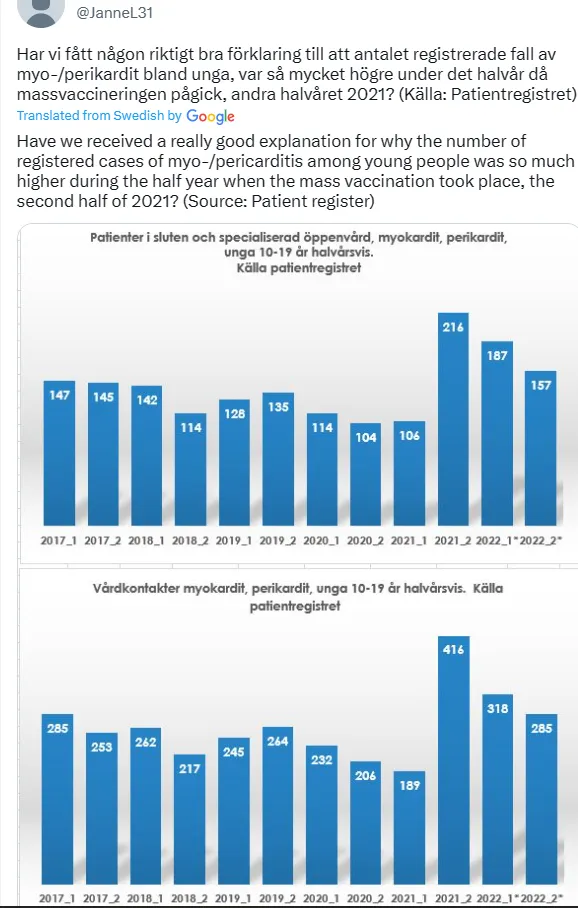
Notice that there is no spike in myocarditis diagnoses until the second half of 2021. Sweden, notably took a light approach to mitigation measures in 2020. They kept schools open, and they suffered large losses of life in care homes (as did every country) as evidence of a virus that was circulating widely through the population. And yet, there is no uptick in myocarditis cases in 2020.
This discrepancy isn’t a result of unawareness of COVID related heart issues as some have proposed because in 2020 the hysteria that surrounded COVID and the heart in 2020 was at a fever pitch. Viral videos from China of people suddenly collapsing, and the very bad German cardiac MRI paper I referenced earlier meant that everyone was looking for a tsunami of COVID heart disease. It just never materialized in the real world.
This data that was known to Swedish authorities in 2021, but not publicized to my knowledge, may have been why the Moderna vaccine with 3x the dose of mrna than Pfizer was banned for anyone < 30 years of age in the Fall of 2021 in Sweden.
The other dataset from last week comes from an epidemiological study that sought to understand the differences in prognosis between COVID19 myocarditis and vaccine myocarditis. The epidemiologists involved clearly were unaware about the issues related to the validity of the diagnosis of COVID19 myocarditis compared to vaccine myocarditis, and to top it off, were unable to specify simple things like what the severity or type of the numerically tiny primary outcome events (heart failure) they did find. As a study of prognosis of COVID vs. vaccine myocarditis, it’s a flimsy paper that is of zero clinical value. What is interesting about the study, despite the study authors admonishments not to look, is the number of vaccine associated myocarditis cases picked up during the study period1.
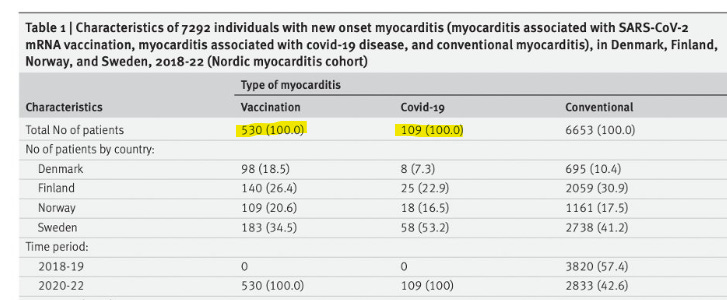
There were almost 5 times as many vaccine myocarditis cases as there were “COVID19 myocarditis” cases in the time window in Scandinavia that was studied. The study authors caution against making a comparison about rates of vaccine vs. covid myocarditis using these numbers because no attempt to present any denominators for covid infections or people vaccinated is given, but given the multiple other rigorous datasets that have shown spikes in vaccine myocarditis cases after the vaccine and not COVID, it’s hard not to notice that over a common number of years studied, there are a lot more vaccine myocarditis cases being diagnosed.
And so we have a tale of two countries.
One that observed a spike in a novel serious adverse event primarily in young healthy males in the Fall of 2021, and chose to restrict the mrna vaccine that caused the most myocarditis to anyone < 30 years of age, and the other country that in February of 2023 still thinks heart problems after COVID 19 is five times more likely than vaccine myocarditis and recommends all COVID vaccines to everyone over 6 months of age.
If no one was paying attention to what the CDC said it wouldn’t really matter, but apparently epidemiologists and others with a weak handle on reality are still mandating vaccines for college kids.
It is well beyond time for these mandates to end, and well beyond time to strip the powers of the innumerate public health hypochondriacs that are running things. There’s at least a semblance of a debate to have about what powers competent public health authorities should have over society, but there can be little argument that inmates should not be running the asylum.
Anish Koka is a Cardiologist. Follow him on twitter @anish_koka
I have to make the obligatory post-script here that I oversaw the administration of hundreds of mrna vaccines starting in March of 2021 in my cardiology clinic. The vaccine efficacy data for the original data was from thousands of patients and I certainly felt given the devastation wreaked on many of my patients in 2020 that the vaccines were the best chance of avoiding morbidity and mortality. The process to get the vaccines from the city department of health was a somewhat arduous 3 month process, and once the vaccines were on hand, there were daily reporting requirements that I dutifully performed for the many months we were administering vaccines. To accommodate the rush of patients, employees, volunteers, and conscripted children worked multiple weekends to administer the vaccines. So I’m especially disgusted by medical colleagues who label any concerns registered about vaccine adverse events as “anti-vaxx”. Registering concern over a vaccine adverse event does not make doctors or patients “anti-vaxx”. It makes them pro-vaxx!
Footnote:
- Recall that vaccine myocarditis cases are straightforward, usually previously healthy young men complaining of chest pain who have evidence of cardiac muscle cell necrosis and supporting cardiac imaging, while COVID myocarditis cases are almost always older, very ill hospitalized patients with pre-existing (sometimes undiagnosed) cardiac disease who have myocardial injury related to the stress of the primary diagnosis. The other COVID19 related myocarditis is not acute myocarditis, but an autoimmune condition that usually occurs months after recovery from COVID called MIS-C myocarditis. Important to note this entity has a lot of overlapping features with an autoimmune diagnosis called Kawasaki’s, and is now so rare that the CDC no longer tracks it.
Categories: Medical Practice









I don’t disagree that there is decent evidence that myocarditis occurs after some mRNA vaccine administration. But it is a very low number. Having said that, given 1) the now endemic nature of the virus in society, 2) the fact that COVID vaccine mandates are unenforceable in a regulatory and practical sense and 3) we have non mRNA based vaccines, I think it’s fine to suggest alternate (or no) vaccines for males aged say 14-28.