
BY ANISH KOKA
The All-in podcast is a fairly popular show that features successful silicon valley investors commenting about everything worth commenting on from politics to health. The group has good chemistry and interesting insights that breaks the mold of the usual tribal politics that controls legacy media analysis of current events.
Last week, the podcast touched on a topic I spend a fair amount of time on: Cardiology.
Brad Gerstner, who is actually a guest host for this particular episode starts off by referencing something called Heartflow to evaluate the heart that has been recommended by one of the other hosts: Chamath Palihapitiya. Brad apparently asked his primary care physician about Heartflow and was instead directed to get a calcium scan.
Heartflow is a proprietary technology that purports to evaluate the presence of significant narrowing in the coronary arteries just by doing a heart CT scan. A calcium score is a low-dose CT scan used to identify the presence of calcium in coronary vessels.
The segment ends with a recommendation for everyone over the age of 40 to get some type of heart scan, so I thought it would be worth reviewing some of the main claims.
Question 1. Does Brad need a calcium scan?
Brad notes that his primary care physician told him he was young, fit, and had a low bad cholesterol (LDL) and needed a calcium scan rather than a heart flow scan. The answer to this question and the questions to follow depend on what outcome Brad is looking for. If the goal is to feel happier knowing if he has coronary calcium than the resounding answer is to get the calcium scan. But if the goal is to live longer and healthier, there is nothing to suggest a calcium scan will help. Most cardiologists believe that the lower the LDL, the better cardiovascular outcomes are. So if a calcium scan convinces Brad to NOT lower his LDL further either naturally or with medications, a calcium scan may be detrimental.
We have zero evidence to suggest patients who get calcium scans lower their risk of future mortality.
Question 2. Does Brad need a Heartflow scan?
Heartflow is a California based company that claims to be able to identify heart vessels leading to a lack of blood to the heart muscle that need coronary stents to fix. Ordinarily this determination is done with a combination of tests that include a stress test and an invasive heart catheterization that involves a catheter being snaked into the heart. Heartflow puports to do all of this with a single 20 minute CAT scan that only involves placement of a peripheral IV using artificial intelligence/machine learning. The evidence to support the use of Heartflow comes mostly from small studies that show no difference in outcomes relative to the standard of care in relatively low risk populations. I could probably use a theragun based AI aproach in 500 carefully selected patients and show no difference in clinical outcomes to the standard of care. This is because the absolute risk of bad clinical events is too low for the size of studies generally being performed. You would need larger numbers to show small differences in outcomes and the Heartflow trials don’t have large numbers – which is convenient when you need series B funding. The small trials do still provide some interesting data about how Heartflow peforms.
The image below from this “positive” Heartflow study shows that almost a quarter of patients who did not have a significant narrowing in their arteries were judged to have a significant narrowing based on Heartflow. And regardless of whether you have a 26-50% narrowing or a 51-70% narrowing, you have a 1 in 4 chance Heartflow will say there’s a problem (when there isn’t).
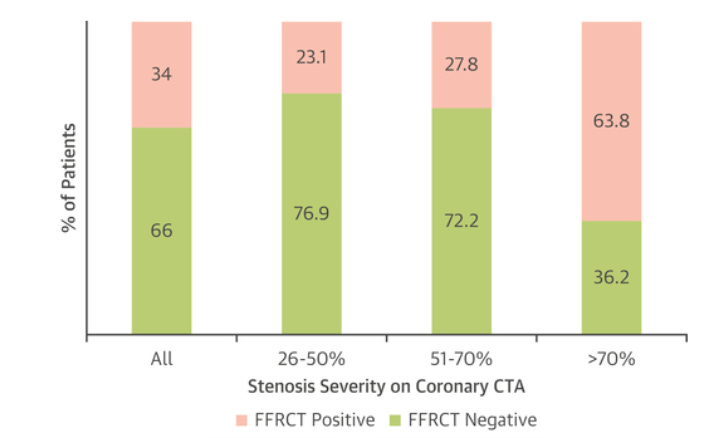
So if Brad wants a pretty picture with some numbers attached to make him feel good, he should definitely pony up a few thousand dollars for a Heartflow scan.
Question 3. Will Heartflow or Calcium scans save lives if deployed broadly in the population?
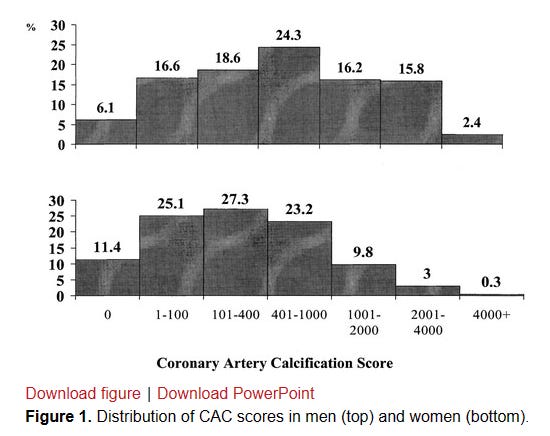
While it seems intuitively obvious that doing more tests to find heart disease will decrease the likelihood of dying from heart disease, the reality is anything but obvious. The history of diagnostic testing for coronary disease shows that we are better and better at identifying disease, but simply identifying coronary plaque isn’t the home run people think because of how ubiquitous the development of coronary plaque is in humans. By the age of 60 it is only the small minority of men and women who have no coronary calcium present (6% of older men, 11% of older women).
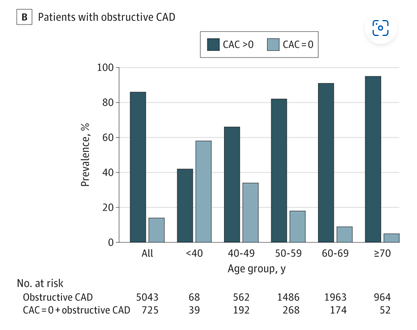
To make matters even more complicated, plaque in younger patients may be non-calcified and invisible to CT-calcium scans. A calcium score of 0 in a younger patient could provide a false sense of security. In the figure below, almost 60% of patients with “obstructive CAD” had a Calcium score of 0 !
Whether or not discovering and treating “obstructive CAD” as defined in the study is beneficial is another complex topic with much nuance.
And lastly, there’s a potential for harm driven by overdiagnosing coronary disease! Every cardiologist that has seen enough patients has a story of a patient with an elevated asymptomatic calcium score that ends up with a disastrous outcome from a cardiac catheterization. The field of interventional cardiology has a remarkable safety profile but the rate of severe complications related to the procedure alone is not zero.
Summary
Calcium scans and HeartFlow are interesting tools, but proponents are well out of their depth to think a universal screening approach using these tools will be beneficial.
The problem here is that these mostly middle aged men discussing the topic are appropriately concerned about the most likely cause of their early demise : heart disease. I’ve written a number of times about the scourge of heart disease in men. It can strike suddenly and without any warning, even in the apparently healthy. The absolute risk of men dying due to their heart giving out is ~ 1/600 in men aged 35-44, ~1/250 in men aged 45-54, ~1/100 in men aged 55-64.
This is enough death to strike fear into the hearts of the healthy, and provides ample opportunity to make billions selling men on the keys to cheating death.
If this topic piques your interest, and you want to dive even deeper, tune in tomorrow, July 16th at 1 pm EST to hear a discussion with cardiologists and other experts on Twitter!
Anish Koka is a cardiologist. Follow him @anish_koka on twitter.
Rough transcript of all-in-pod provided by YouTube:
1:31:50
about this pod is we cover everything from science to politics and and chamoth last year
1:31:56
um you know in his biohacking series told us all to get pre-nuvo scans which I did which is interesting and I think I
1:32:02
don’t know maybe 10 people have have sent you notes and said hey you helped me discover a tumor you know really
1:32:09
amazing well so this year and I did that um you know this year you’ve been talking a lot about heart flow so I said
1:32:15
to my general practitioner at my annual checkup hey I want to do this heart flow and she said oh you don’t need to do a
1:32:21
heart flow your ldls all your stuff looks real wait wait wait wait wait wait wait wait you have a female GP
1:32:27
uh she’s fantastic fantastic Stanford educated really terrific I don’t care
1:32:32
where she went who does the prostate test he does Hey listen it’s it you know
1:32:38
the perks that come check in the PSAs I mean no but seriously you have it really I do I do that’s a level of intimacy I
1:32:46
didn’t expect from you wow and so you know but what I found interesting is
1:32:51
when I suggested I get the heart flow she said oh you don’t need it Etc your ldls are low you’re very fit and she
1:32:59
said but on second you know maybe you could go get this calcium score test right
1:33:04
um I didn’t know anything about this but you know I did a little quick research and it turns out a big Jam of study in
1:33:10
2017 over 50 percent of men and women over the age of 40 Carrie plaque
1:33:16
plaque’s the number one killer it’s a source of heart uh disease and and heart attacks and as Chamas been talking about
1:33:23
there’s you know a a prophylactic called Statin which is basically like a supplement very little downside no
1:33:30
long-term downside effects but it immediately starts cutting down the amount of fatty cells and and and plaque
1:33:36
that’s carried in your blood so I thought it was interesting I went and I had chemath uh as you know the core the
1:33:42
coronary calcium scan it takes five minutes it costs between a hundred and four hundred dollars the fact that we
1:33:47
don’t have every person taking this over 40 is crazy and Frontline doctors should all be prescribed in it but it
1:33:53
particularly if there’s family history sorry but did you also do a contrast CT with heart flow yeah so I started with
1:33:59
the calcium score 150 bucks over at Stanford took five minutes and you know it told me uh you know which wasn’t
1:34:06
terribly surprising I was one of the 50 percent that did carry some level of calcium so it was called a non-zero
1:34:13
score and then what they suggest is because you have a non-zero score you get this
1:34:19
you know chamoth you told me go do the contrast CT which then will image what
1:34:25
this looks like actually in your artery so this past week in Boston I did the contrast CT again this took 10 minutes
1:34:32
non-invasive like you know it just they run you into it invasive because you have to put the dye so they put yes so
1:34:41
so a tiny bit I I suppose they shoot a little die into you but you know um uh it didn’t feel like anything
1:34:48
I was in and out of the of the place in 40 minutes and what it found is you know
1:34:54
fortunately that very little of this calcium had turned into what they call stenosis any narrowing of of the
1:35:01
arteries okay but then it gave you just a very clear picture that if you are one
1:35:07
of the 50 who carry plaque over the age of 40 you should be on a prophylactic
1:35:13
Statin so it’s chamat knows I signed up to 10 milligrams of crestar which I’m taking daily has had zero you know zero
1:35:20
adverse consequences and in two or three months they’ll test the amount of you know we’ll revisit this calcium score
1:35:28
um but when I talked to the head of Cardiology what was so interesting he said every one of his friends over the
1:35:34
age of 40 he has them do this calcium coronary scan it’s so cheap and if
1:35:39
they’re zero on their calcium reading that that’s the end of the line but if they have a non-zero reading then he’ll
1:35:45
do the the CT coronary scan which is again very cheap more expensive than the
1:35:51
calcium test but very cheap and when you think about the cost of the patients in this country right in our health care
1:35:58
System due to heart disease and when you think about the needless lives cut short I was shocked how easy all of this was
1:36:07
and how empowered I feel by the data and how fortunate I feel that I’m actually
1:36:12
taking a supplement I call it a supplement instead of statins because I think Statin has some spooky name it
1:36:17
sounds to me like a better supplement than any vitamins I can take and you know it’s reducing the ldls or these
1:36:24
fatties in your you know in your blood and I’ll keep you posted but I was very grateful and you know as you know I
1:36:29
posted it in our thread and I think all the besties you know we saw responses out of a bunch of folks in the thread
1:36:35
this week are going to go get their calcium uh you know coronary scan and I
1:36:41
I think it should be Common Sense on the front lines for people over 40 particularly if there’s any family
1:36:46
history go get this calcium test done this summer while you have a little extra time there you have it folks
1:36:53
100 to 400 could save your life calcium coronary scan Brad gerstner thanks so much for science Corner this week
Categories: Medical Practice








