I know, I should be writing about hot topics like monkeypox or the baby formula shortage, but, c’mon, Congress held hearings last week about UFOs – the first in 50 years! I mean, I followed Project Blue Book in the 1970’s, watched “The X-Files” in the 1990’s, and have seen UFO videos on YouTube. If Congress is starting to take UFO’s seriously, how could I not?
And for those of you who don’t see any possible connection to healthcare (except for those unpleasant alien probes…), let me put it to you this way: by 2050, is it more likely that:
We’ll know what UFOs actually are;
We’ll have fundamentally reformed the U.S. healthcare system.
One of my favorite movies is The Princess Bride. Among the many great quotes is one from Inigo Montoya, who becomes frustrated when the evil Vizzini keeps using “inconceivable” to describe events that were clearly actually taking place. “You keep using that word,” Inigo finally says. “I do not think it means what you think it means.”
So it is for most of us with the word “innovation” – especially in healthcare.
What started thinking me about this is an opinion piece by Alex Amouyel: Innovation Doesn’t Mean What You Think It Does. Ms. Amouyel is the Executive Director of Solve, an MIT initiative whose mission is “to drive innovation to solve world challenges.” It sees itself as “a marketplace for social impact innovation.”
In her article, Ms. Amouyel notes that traditional definitions of innovation focus on the use of novelty to create wealth. She doesn’t dispute that view, as long as “wealth” includes the less traditional “community wealth,” which includes “broadly shared economic prosperity, racial equity, and ecological sustainability.” I suspect that innovators like Jeff Bezos or Elon Musk don’t ascribe to that view of innovation.
Ms. Amouyel’s view is: “For me, innovation is about solving problems. And if innovation is about solving problems, what problems you are solving and who is setting about solving them is key.” She notes the multiplicity and difficulty of both global and community-level problems that we face, and urges: “Most urgently, we should zero in on problems that affect the most underserved among us.”
Abortion rights continue to be one of the most heated issues in American politics, super-fueled by last week’s leak of a draft Supreme Court opinion that would overturn 1973’s Roe v. Wade and return the issue to the states to decide.
I’ll leave it to others more qualified than me – women, for example — to weigh in on abortion itself, but I want to talk about how abortion pills are going to force changes to our healthcare system that many may not be ready for.
Although the stereotype of abortions is a procedure done by a physician in an office/clinic, the majority of abortions in the U.S. are now done through the use of abortion pills. It is a two step process, and the two medications must be prescribed by a physician. Until last December, women were required to see a physician in person, but the FDA permanently lifted those requirements, following a temporary waiver during the pandemic. The pills are considered both highly effective and safe. There are startups, like Hey Jane and Just the Pill, that specialize in them.
The states that have been passing various abortion bans have not ignored the loophole that abortion pills represent. There are a variety of restrictions that have been enacted, such as requiring in-person visits to outright banning use of telehealth for them. In those states, some women have opted to travel out of state to do the telehealth visit and/or to receive the pills via the mail.
If you went to business school, or perhaps did graduate work in statistics, you may have heard of survivor bias (AKA, survivorship bias or survival bias). To grossly simplify, we know about the things that we know about, the things that survived long enough for us to learn from. Failures tend to be ignored — if we are even aware of them.
This, of course, makes me think of healthcare. Not so much about the patients who survive versus those who do not, but about the people who come to the healthcare system to be patients versus those who don’t. It has a “patient bias.”
Survivor bias has a great origin story, even if it may not be entirely true and probably gives too much credit to one person. It goes back to World War II, to mathematician Abraham Wald, who was working in a high-powered classified program called the Statistical Research Group (SRG).
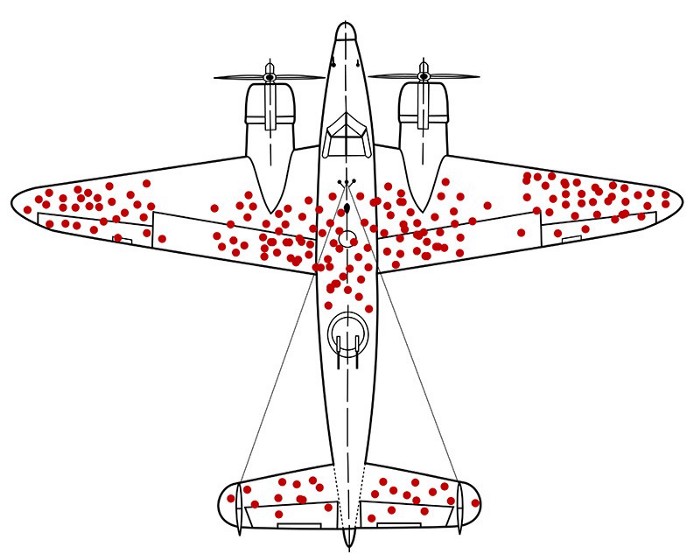
One of the hard questions SRG was asked was how best to armor airplanes. It’s a trade-off: the more armor, the better the protection against anti-aircraft weapons, but the more armor, slower the plane and the fewer bombs it can carry. They had reams of data about bullet holes in returning airplanes, so they (thought they) knew which parts of the airplanes were the most vulnerable.
Dr. Wald’s great insight was, wait — what about all the planes that aren’t returning? The ones whose data we’re looking at are the ones that survived long enough to make it back. The real question was: where are the “missing holes”? E.g., what was the data from the planes that did not return?
Joining Matthew Holt (@boltyboy) on #THCBGang on April 28 for an hour of topical and sometime combative conversation on what’s happening in health care were: THCB regular writer and ponderer of odd juxtapositions Kim Bellard (@kimbbellard); medical historian Mike Magee (@drmikemagee); patient safety expert and all around wit Michael Millenson (@mlmillenson) & Principal of Worksite Health Advisors Brian Klepper (@bklepper1). Matthew had COVID so didn’t do much & Kim ran the show. Lots of discussion on telehealth, primary care, private equity and much more…
You can see the video below & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.
America loves innovation. We prize creativity. We honor inventors. We are the nation of Thomas Edison, Henry Ford, Jonas Salk, Steve Jobs, and Stephen Spielberg, to name a few luminaries. Silicon Valley is the center of the tech world, Hollywood sets the cultural tone for the world, and Wall Street is preeminent in the financial world. Our intellectual property protection for all that innovation is the envy of the world.
But, as it turns out, maybe not so much. If there’s any doubt, just look at our healthcare system.
———
Matt Richtel writes in The New York Times “We Have a Creativity Problem.” He reports on research from Katz, et. alia that analyzes not just what we say about creative people, but our implicit impressions and biases about them. Long story short, we may say people are creative but that doesn’t mean we like them or would want to hire them, and how creative we think they depend on what they are creative about.
“People actually have strong associations between the concept of creativity and other negative associations like vomit and poison,” Jack Goncalo, a business professor at the University of Illinois at Urbana-Champaign and the lead author on the new study, told Mr. Richtel.
Vomit and poison?
A previous (2012) study by the same team focused on why we say we value creativity but often reject creative ideas. “We have an implicit belief the status quo is safe,” Jennifer Mueller, a professor at the University of San Diego and a lead author on the 2012 paper, told Mr. Richtel. “Novel ideas have almost no upside for a middle manager — almost none, The goal of a middle manager is meeting metrics of an existing paradigm.”
You’ve been there. You’ve seen that. You’ve probably blocked a few creative ideas yourself.
The 2012 research pointed out: “Our findings imply a deep irony. Prior research shows that uncertainty spurs the search for and generation of creative ideas, yet our findings reveal that uncertainty also makes us less able to recognize creativity, perhaps when we need it most. Moreover, “people may be reluctant to admit that they do not want creativity; hence, the bias against creativity may be particularly slippery to diagnose.”
In the new study, participants were given two identical descriptions of a potential job candidate, except that one of the candidates had demonstrated creativity in designing running shoes, but the other in designing sex toys (the researchers note: “the pornography industry plays a significant role in the refinement, commercialization, and broad dissemination of innovative new technologies”). The participants explicitly rated the latter candidate as less creative, although their implicit ratings showed equal ratings.
The researchers concluded:
Collectively, the findings strongly support our contention that implicit impressions of creativity can readily form, be differentiated from a traditional explicit measure, and uniquely predict downstream judgment, such as hiring decisions, that might be relevant in an organizational context.
This matters, they say, because: “the findings of study 4 seem to square with real world examples of highly creative people who were ignored until well after their death because their work was too controversial in its time to be recognized as a creative contribution…”
We think we know robots, from the old school Robbie the Robot to the beloved R2-D2/C-3PO to the acrobatic Boston Dynamics robots or the very human-like Westworld ones. But you have to love those scientists: they keep coming up with new versions, ones that shatter our preconceptions. Two, in particular, caught my attention, in part because both expect to have health care applications, and in part because of how they’re described.
Hint: the marketing people are going to have some work to do on the names.
———–
Let’s start with the robot called by its creators – a team at The Chinese University of Hong Kong — a “magnetic slime robot,” which some in the press have referred to as a “magnetic turd robot” (see what I mean about the names?). It has what are called “visco-elastic properties,” which co-creator Professor Li Zhang explained means “sometimes it behaves like a solid, sometimes it behaves like a liquid…When you touch it very quickly it behaves like a solid. When you touch it gently and slowly it behaves like a liquid”
The slime is made from a polymer called polyvinyl alcohol, borax, and particles of neodymium magnet. The magnetic particles allow it to be controlled by other magnets, but also are toxic, so researchers added a protective layer of silica, which would, in theory, allow it to be ingested (although Professor Zhang warned: “The safety [would] also strongly depend on how long you would keep them inside of your body.”).
The big advantage of the slime is that it can easily deform and travel through very tight spaces. The researchers believe it is capable of “grasping solid objects, swallowing and transporting harmful things, human motion monitoring, and circuit switching and repair.” It even has self-healing properties.
Watch it in action:
In the video, among other tasks, the slime surrounds a small battery; researchers see using the slime to assist when someone swallows one. “To avoid toxic electrolytes leak[ing] out, we can maybe use this kind of slime robot to do an encapsulation, to form some kind of inert coating,” Professor Zhang said.
As fate would have it, the news of the discovery hit the on April 1st, leading some to think it was an April Fool’s joke, which the researchers insist it is not. Others have compared the magnetic slime to Flubber or Venom, but we’ll have to hope we make better use of it.
It is not yet autonomous, so some would argue it is not actually a robot, but Professor Zhang insists, “The ultimate goal is to deploy it like a robot.”
———-
If magnetic slime/turd robots don’t do it for you, how about a “magnetic tentacle robot” – which some have deemed a “snakelike” robot? This one comes from researchers at the STORM Lab at the University of Leeds. STORM Lab’s mission is:
We strive to enable earlier diagnosis, wider screening and more effective treatment for life-threatening diseases such as cancer…We do so by creating affordable and intelligent robotic solutions that can improve the quality of life for people undergoing flexible endoscopy and laparoscopic surgery in settings with limited access to healthcare infrastructures.
In this particular case, rather than using traditional bronchoscopes, which might have a diameter of 3.5 – 4 millimeters and which are guided by physicians, the magnetic tenacle robot offers a smaller, more flexible, and autonomous option. Professor Pietro Valdastri, the STORM Lab Director, explained:
A magnetic tentacle robot or catheter that measures 2 millimetres and whose shape can be magnetically controlled to conform to the bronchial tree anatomy can reach most areas of the lung, and would be an important clinical tool in the investigation and treatment of possible lung cancer and other lung diseases.
Moreover, “Our system uses an autonomous magnetic guidance system which does away for the need for patients to be X-rayed while the procedure is carried out.” A patient-specific route, based on pre-operative scans, would be programmed into the robotic system. It could then inspect suspicious lesions or even deliver drugs.
Dr. Cecillia Pompili, a thoracic surgeon who was a member of them team, says: “This new technology will allow to diagnose and treat lung cancer more reliably and safely, guiding the instruments at the periphery of the lungs without the use of additional X-rays.”
The robot was tested on a 3D replica of a bronchial tree, and will next be tested on lungs from a cadaver. It will likely take several years to reach clinical settings. The team has also created a prototype of a low-cost endoscope and a robotic colonoscopy system, among other things.
We demonstrate that the proposed approach can perform less invasive navigation and more accurate targeting, compared with previously proposed magnetic catheterization techniques… we believe that atraumatic autonomous exploration of a wide range of anatomical features will be possible, with the potential to reduce trauma and improve diagnostic yield.”
“It’s creepy,” Professor Valdastri admitted to The Washington Post. “But my goal … is to find a way to reach as deep as possible inside the human body in the least invasive way as possible… Depending on where a tumor is, this may be the only way to reach [it] successfully.”
Nitish V. Thakor, a professor of biomedical engineering at Johns Hopkins University, told The Post: I can imagine a future where a full CAT scan is done of the lungs, and the surgeon sits down on a computer and lays out this navigation path of this kind of a snake robot and says: ‘Go get it.’ ” He also sees potential for uses outside the lungs, such as in the heart.
Similarly, Dr. Janani S. Reisenauer, a surgeon at The Mayo Clinic, declared to The Post: “If it’s a small, maneuverable autonomous system that can get out there and then do something when it’s out there, that would be revolutionary.”
———-
Personally, I’m still holding out hope for nanoparticles, but these kinds of soft, flexible robots could be important until we get there. Sure, maybe people will be reluctant to be told they have to ingest magnetic slime – much less a magnetic turd – or have a snakelike robot put down their throats, but it may beat having a scope inserted or being cut open.
The researchers can keep working on the robots; others of us can work on better names.
Kim is a former emarketing exec at a major Blues plan, editor of the late & lamented Tincture.io, and now regular THCB contributor.
Joining Matthew Holt (@boltyboy) on #THCBGang on March 24 for an hour of topical and sometime combative conversation on what’s happening in health care and beyond were fierce patient activist Casey Quinlan (@MightyCasey); patient safety expert and all around wit Michael Millenson (@MLMillenson); THCB regular writer and ponderer of odd juxtapositions Kim Bellard (@kimbbellard); and back from his travels in Mexico and medical historian Mike Magee (@drmikemagee).
Special guest this week was population health and primary care expert Ines Vigil, who developed that program at Johns Hopkins but now hangs her hat at Clarify Health &is the author of Population Health Analytics. We dived deep into what populations health means. What we need to do to make it work and whether it’s real or not!
You can see the video below live (and later archived) & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.
Joining Matthew Holt (@boltyboy) on #THCBGang at 1pm PT 4pm ET Thursday for an hour of topical and sometime combative conversation on what’s happening in health care and beyond will be: fierce patient activist Casey Quinlan (@MightyCasey); patient safety expert and all around wit Michael Millenson (@MLMillenson); THCB regular writer and ponderer of odd juxtapositions Kim Bellard (@kimbbellard); and policy consultant/author Rosemarie Day (@Rosemarie_Day1).
The video will be below. If you’d rather listen to the episode, the audio is preserved from Friday as a weekly podcast available on our iTunes & Spotify channels
Like many of you, I have been intently following the war in Ukraine, cheering for President Zelensky and the Ukrainian people, while hoping it doesn’t end up in WW3. I thought about trying to write about it, then I saw that Raspberry Pi just turned ten, and I thought, yeah, that’s more my speed.
And, of course, easier to relate to healthcare.
For most of us, a computer is our smartphone, tablet, or laptop. We buy them already designed and built, complete with an operating system and other useful software. There’s an almost unlimited range of other software that can easily be downloaded to run on them. Ease of use is paramount.
This was not always so. If you are of a certain age or have studied the history of computers, you’ll know that in the 1970s and early 1980s, (home) computers came in a kit. You assembled them and figured out what you might want to use them for. Then came Apple and the PC revolution. Our expectations about what computers could do grew as our expectations about what we had to do diminished. Between 2006 and 2011, Eben Upton and his collaborators sought to change this.