
BY ANISH KOKA
A recent CNN article discusses approval of the Moderna Covid-19 vaccine for people ages 6-17. The CDC director acted after its vaccine advisers on the Advisory Committee on Immunization Practices voted unanimously to support the two dose Moderna COVID-19 vaccine for kids in this age group. The goal per CDC director Walensky was to “protect our children and teens from the complications of severe COVID-19 disease”

The elephant in the room that the CDC advisory group addressed is the risk of myocarditis from the vaccines that has been widely reported since April of 2021 by multiple groups and countries.
There is a risk of myocarditis/pericarditis after both messenger RNA Covid-19 vaccines, most cases have prompt improvement in symptoms. A follow up survey suggests most fully recovered from myocarditis,” said Dr. Helen Keipp Talbot
She added that myocarditis after vaccination has been generally mild compared to those who developed myocarditis after getting sick from Covid-19
The first statement about the prompt recovery noted is technically true, but there is some important context that’s missing. The reader, and non-cardiologists may be lead to believe by the way Dr. Talbot, an infectious disease physician, frames this complication that the myocarditis that occurs after a vaccine is similar to a mild cold. This is absolutely not the case. Until myocarditis began happening after the messenger RNA vaccines, myocarditis in children and adult was regarded as a severe, potentially life threatening condition. The experience with vaccine myocarditis to date in hospitals has demonstrated that this particular syndrome does not appear to be as severe as classical myocarditis, but parents should not be under the mistaken impression this is a mild phenomenon resembling a cold.
The diagnosis of myocarditis in previously healthy children means that myocardial damage, or myocardial cell death has occurred. Again, the amount of damage seen is less than what is typically seen in conventional, classic myocarditis, but the autoimmune process that creates the damage in the heart typically will cause severe pain, and requires a hospital stay for monitoring, and cardiac testing the vast majority of the time.
Here’s a thread from a very pro-vaccine parent , and her twitter thread describing her child‘a experience with vaccine myocarditis. Her son recovered just like the CNN expert said, but to represent this best-case scenario as mild is wrong.
As the thread details, the story doesn’t end after the hospital stay. The recommendation after recovery from myocarditis is to avoid strenuous activity for 3-6 months after recovery from the acute process to avoid the theoretical risk of precipitating a lethal cardiac arrhythmia while the heart is recovering/scarring. Studies have also demonstrated that most cases of vaccine myocarditis are associated with a scar that is seen on cardiac MRI. (More on this later in the blog) The amount of scar is less than that seen with classical myocarditis, but at best, it is uncertain what the prognosis of these scars are in children long term. There are also specialist visits as well as the financial burden that even insured parents have to deal with related to the after-care of myocarditis. To date, the vaccine compensation injury program has not seen fit to provide any renumeration to those judged injured from the vaccine.
So no, the issues related to vaccine myocarditis are not consistent with the adjective ‘mild’ or any statements that imply this isn’t a serious event that you would want to avoid for your child.
The second statement attributed to Dr. Talbot regards the relative seriousness of myocarditis after getting COVID to vaccine related myocarditis. If it were true, this would make the decision about mRNA vaccines for children incredibly easy. Unfortunately, it isn’t so simple. Dr. Talbot is most likely referring to myocarditis that happens in children after a syndrome called MIS-C, an inflammatory condition that is thought to be linked to having had COVID in the past. This is a severe illness that typically is associated with very low pressures (referred to in medical terminology as shock) and can be associated with multiple organs that are dysfunctional, including the heart. This heart dysfunction with MIS-C has come to be known as MIS-C myocarditis.
Generally children recover from MIS-C as well, but it is quite a scary process that again, you would do anything to avoid.
The interesting thing about the three types of myocarditis (classical myocarditis, vaccine myocarditis, and MIS-C myocarditis) is that they are really different with regards to the damage done to the heart. Its also really important to note that the virus that causes COVID is not known to invade the heart muscle. This is why every case series of vaccine myocarditis doesn’t ever have any actual covid-caused- myocarditis. You don’t have to take my word for it — pediatric cardiologist Matthew Oster noted in his presentation to the vaccine advisory board that in his analysis at a quaternary care pediatric hospital, he did not include any cases of acute COVID myocarditis because there were no cases of acute covid myocarditis.
So when people discuss myocarditis in kids related to COVID, they are talking about the myocarditis related to MIS-C that happens well after the acute COVID infection has resolved.
With regards to the cardiac damage meted out by the three different types of myocarditis, as measured by the amount of protein/enzyme leaked from dying cardiac muscle cells (troponin), the good news is that MIS-C myocarditis is associated with almost no cardiac damage. But there is little question the level of cardiac damage that results from the vaccines is nothing that anyone in a non-COVID era would describe as mild.
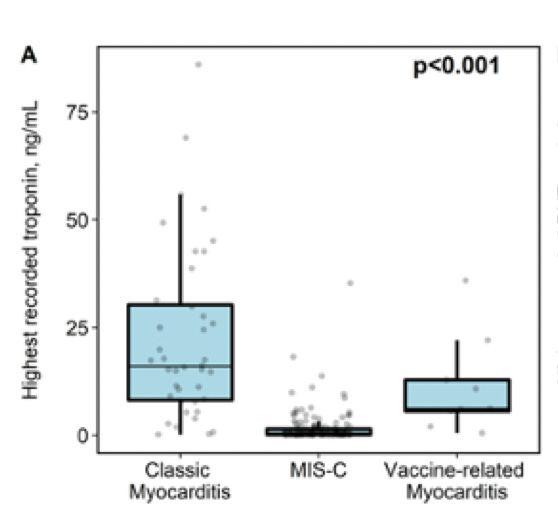
This raises the real possibility that the cardiac dysfunction seen in MIS-C is primarily related to a stress phenomenon that is also described in adult patients during critical illnesses.
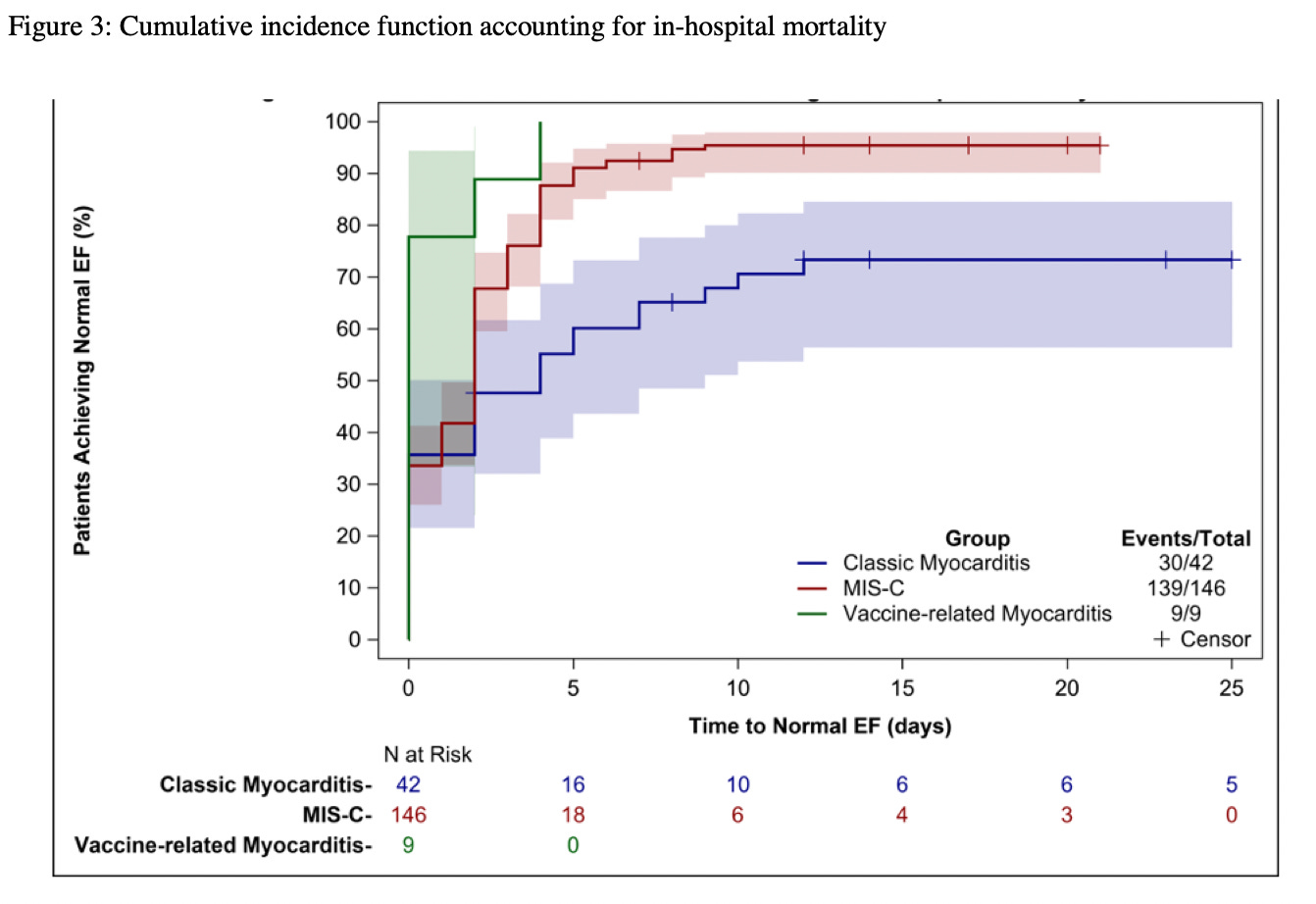
Thankfully the cardiac dysfunction associated with this stress related cardiac dysfunction almost always improves once the critical illness resolves. (Also thankfully, MIS-C is rarely fatal). This is borne out by more data from Dr. Oster and colleagues that shows rapid resolution of heart function for children afflicted with both vaccine and MIS-C associated myocarditis.
Unfortunately, because of the greater cardiac damage seen with the vaccines relative to MIS-C myocarditis, the long term effects as it relates to scar formation in the heart is worse with vaccine myocarditis as it relates to MIS-C myocarditis.
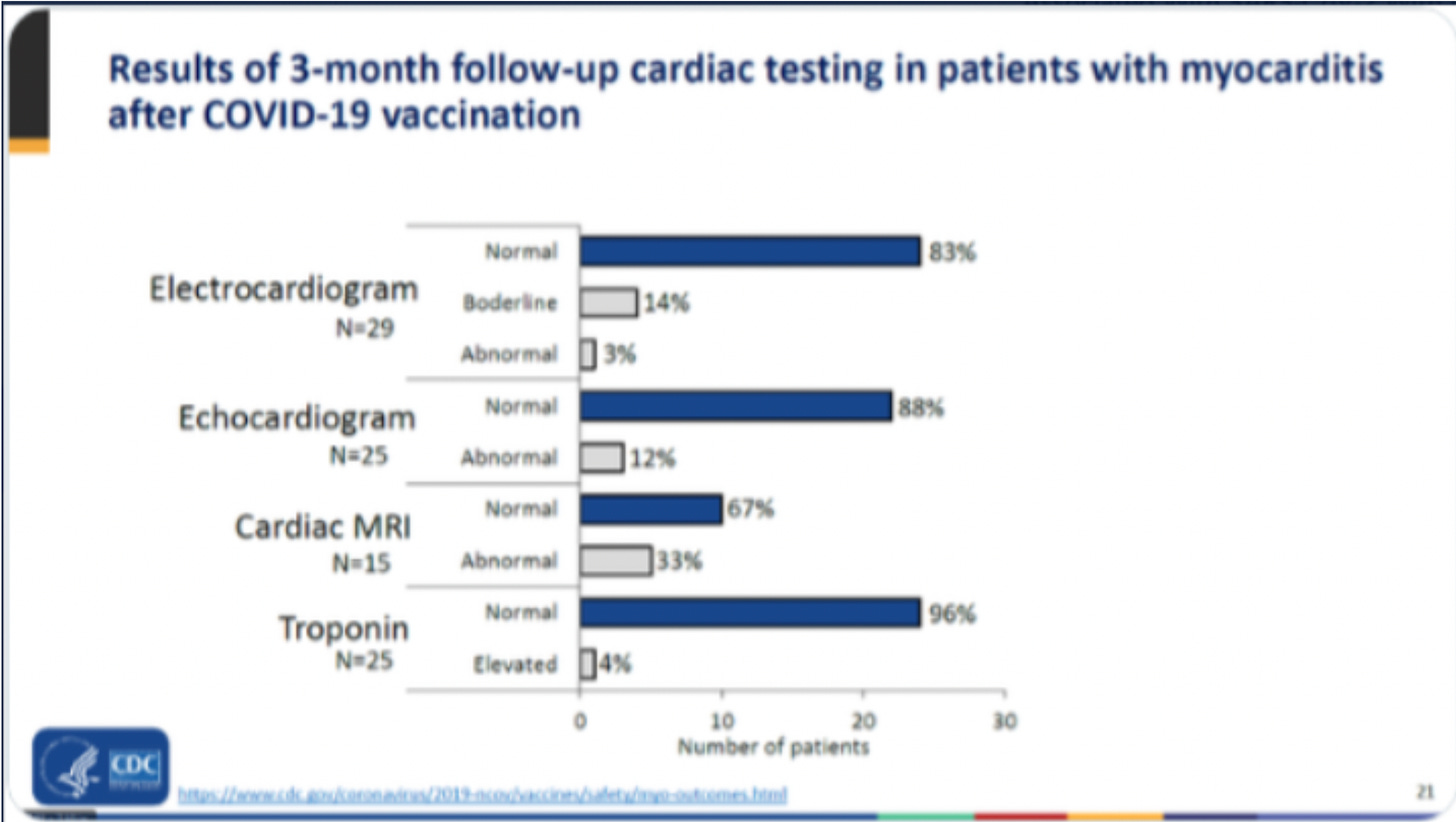
A third of children who get cardiac MRIs after 3 months have evidence of scar on MRI after recovering from vaccine myocarditis, as compared to cardiac MRI studies in MIS-C where no children have evidence of scar.
So if we’re discussing MIS-C myocarditis vs. vaccine myocarditis, there is no question vaccine myocarditis is worse. There’s greater cardiac damage, and there’s a much greater chance of scar development. If CNN’s translation of their expert is correct, suggesting covid related myocarditis is worse than vaccine myocarditis is an incorrect statement.
It is true that MIS-C is a more serious acute illness than vaccine myocarditis, but the article that was written last week fails to comment on the interesting but significant decoupling of MIS-C with prior COVID surges. Specifically there was a massive spike in cases among children in the Fall/Winter, and as per the current CDC data, no expected MIS-C spike has yet emerged.
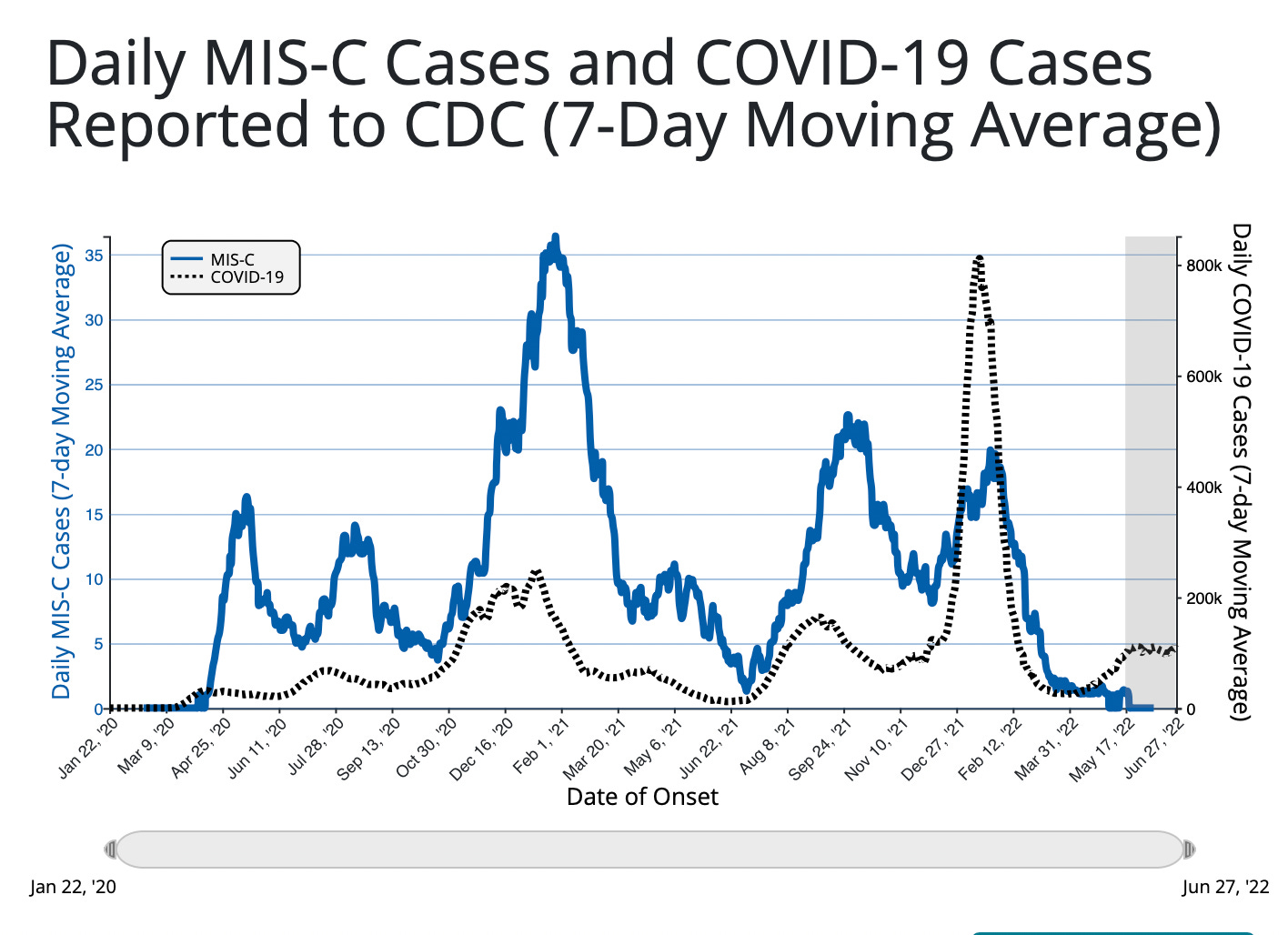
While this raises some important questions about how confident we can be about the causal link between prior COVID infections and MIS-C, it does raise the possibility that the risk to children from COVID is decreasing over time. Some have suggested vaccines in children may be responsible for the decoupling seen, but this is unlikely because the age group that MIS-C afflicts the most (5-11) was largely unvaccinated when the Fall/Winter surge of cases occurred.
The CNN article also doesn’t make any mention of the much higher rates of myocarditis that are seen with the Moderna vaccine as related to the Pfizer vaccine. Moderna has 3 times the amount of vaccine as Pfizer, and multiple studies have demonstrated higher rates of myocarditis, especially after the second dose of the Moderna vaccine. A recent French database suggested rates of myocarditis for Moderna (mrna-1273) that were 3-4 x higher (1/5900 vs 1/21,100) than rates of Pfizer (BNT162b2).
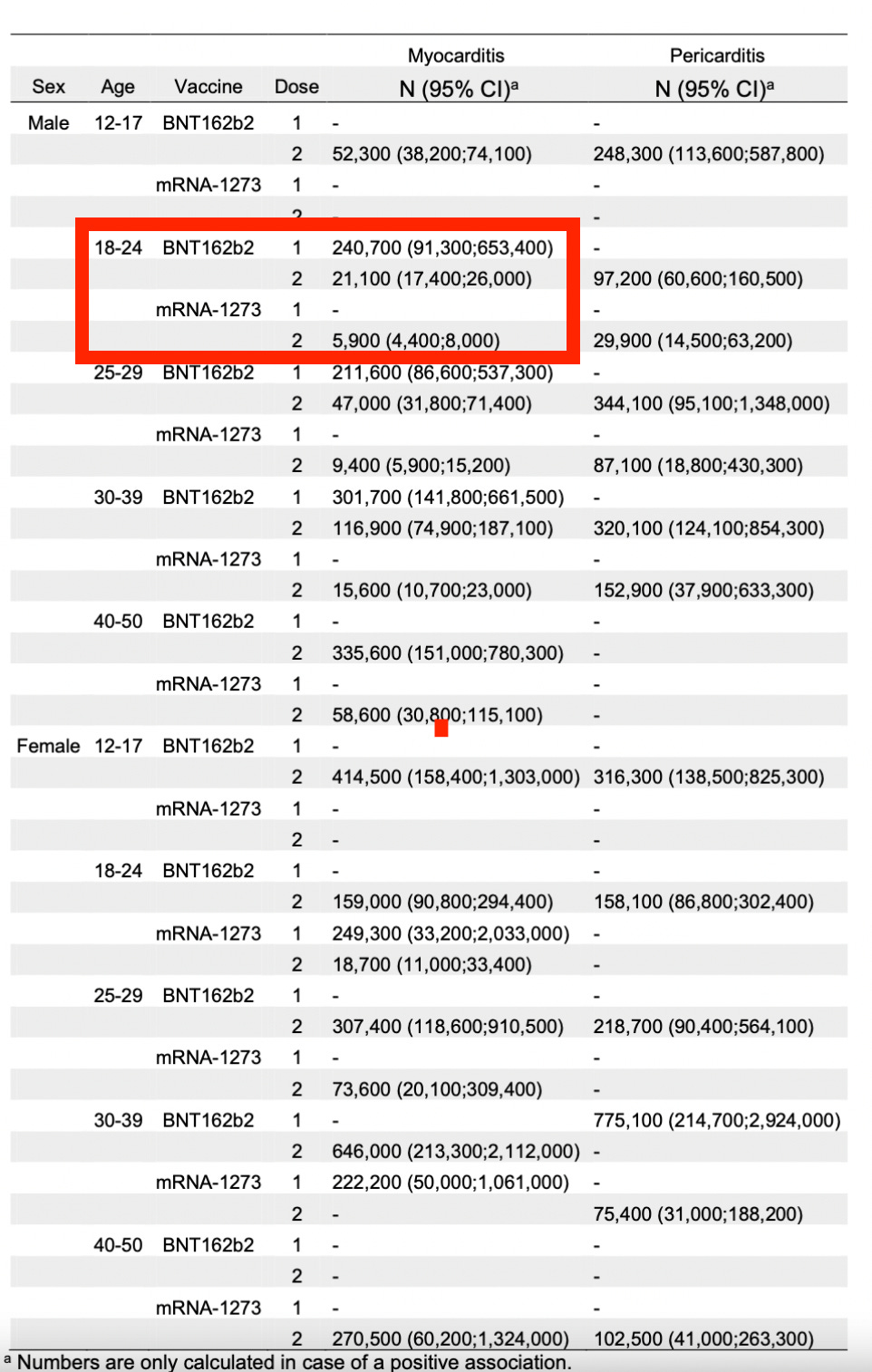
These rates are, of course, with the adult dose of the vaccines, and its likely these rates of myocarditis are lower at the lower doses of vaccine approved for younger age groups, but even if you were convinced of the protective effects of the mrna vaccine for children, why would one choose the vaccine ( Moderna ) that has a much higher adverse event rate of a serious complication?
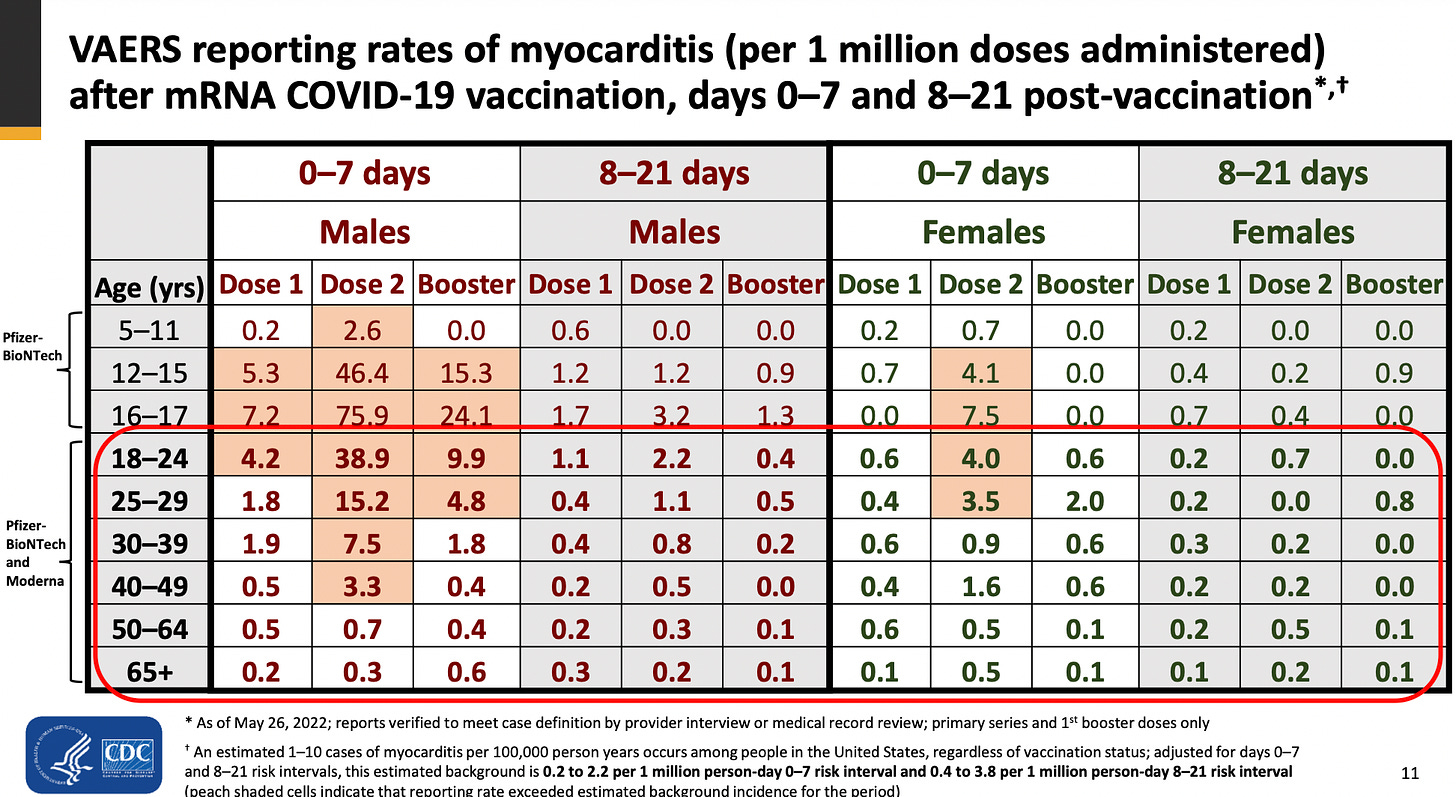
It’s also worth noting that the age group that the CNN article references includes the age group with the highest risk of myocarditis (16-17) as per the CDC’s own data. The orange shaded areas all represent myocarditis rates that are higher than background. Notice that, while there’s a clear peak for 16-17 year old boys, the higher than background rates of myocarditis extends from age 5 to 49.
So CNN does a pretty poor job of doing justice to a very complex topic. Anyone intellectually honest that understands the topic and knows the data would, at best, recommend an alternative vaccine that has a much lower rate of myocarditis. Recent public comments from a Canadian public health authority also channel what many people have been thinking for some time — it seems highly likely that in certain groups at high risk for myocarditis, the risks of a messenger RNA vaccine may be higher than the personal benefit accrued to the individual.
The decision on vaccines in children should be a personal one that’s left to parents, and certainly not one that is defacto forced on them in order for their children to participate in society.
Public health officials that don’t speak like Dr. Moore from Ontario, Canada are destroying their credibility. The expert sources CNN quote to support the CDC decision either don’t understand the topic, or want to keep the message simple to get the public to buy in. Unfortunately, all this is doing is further undermining the credibility of medical professionals and public health institutions. We are failing the public, and it’s embarrassing.
Anish Koka is a Cardiologist. Follow him on twitter @anish_koka
Categories: Medical Practice








