
Tuesday’s announcement about Amazon, Berkshire Hathaway and JPMorgan (A/BH/JPM) was short on details. The three mega-firms will form an independent company that develops solutions, first, for their own companies’ health plans and then, almost certainly, for the larger health care marketplace. But the news reverberated throughout the health care industry as thoroughly as any in recent memory.
Health care organizations were shaken. Bloomberg Markets reported that:
Pharmacy-benefit manager Express Scripts Holding Co. fell as much as 11 percent, the most intraday since April, at the open of U.S. trading Tuesday, while rival CVS Health Corp. dropped as much as 6.4 percent. Health insurers also fell, with Anthem Inc. losing as much as 6.5 percent and Aetna, which is being bought by CVS, sliding as much as 4.3 percent.
As expected, these firms’ stock prices rebounded the next day. But you could interpret the drops as reflections of the perceived fragility of health care companies’ dominance, and traders’ confidence in the potential power of Amazon’s newly announced entity. Legacy health care firms, with their well-earned reputations for relentlessly opaque arrangements and egregious pricing, are vulnerable, especially to proven disruptors who believe that taming health care’s excesses is achievable. Meanwhile, many Americans have come to believe in Amazon’s ability to deliver.
Those who buy health care for employers and unions probably quietly rejoiced at the announcement. For them, the prospect of a group that might actually transform health care would be a breath of fresh air. In my experience at least, the CFOs and benefits managers at employers and unions are acutely aware that they’re being taken advantage of by every health care industry sector. They’re genuinely weary from it, and they’d welcome a solid alternative.
Their health care intentions notwithstanding, the A/BH/JPM group is formidable, representing immense strength and competence. Amazon is an unstoppably proven serial industry innovator, continuing to consolidate its position in the US and in key markets globally. Berkshire Hathaway harbors significant financial strength and a stop-loss unit, US Medical Stop Loss, fluent in underwriting health care risk, which should be handy. In addition to the fact that JPMorgan is the nation’s largest bank, with assets worth nearly $2.5 trillion in 2016, it has a massive list of prospective buyers in its commercial client base.
This triumvirate knows that, in health care, they have an advantage. There are proven but mostly untapped approaches in the market that effectively manage health care clinical, financial and administrative risk, consistently delivering better health outcomes at significantly lower cost. In the main, legacy health care organizations have ignored these solutions, because efficiencies would compromise their financial positions.
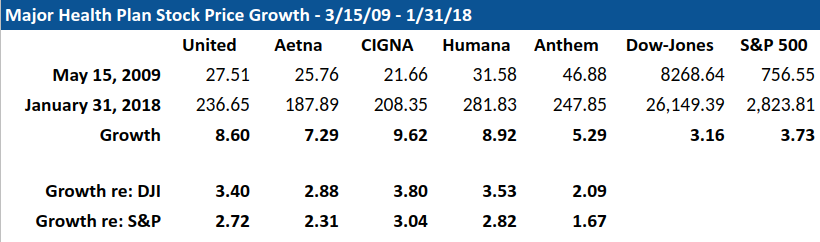
To put this into perspective, consider that, since early 2009, when the Affordable Care Act was passed, the stock prices of the major health plans have grown a spectacular 5.3-9.6 times, 3.7 times the growth of the S&P and 3.2 times the growth of the Dow.
At the end of the day under current fee-for-service arrangements, health care’s legacy organizations make more and have rising value if health care costs more. If they take advantage of readily available solutions that make health care better and cost less, earnings, stock price and market capitalization will all tumble. They’re in a box.
What little we know about Amazon’s intentions indicates that they are ambitious. Presumably they’ll begin by bringing technology tools to bear. That could cover a lot of territory, but assembling and integrating high value narrow networks by identifying the performance of different health care product/service providers seems like a doable and powerful place to begin. High performance vendors exist in a broad swath of high value niches. Arranging these risk management modules under a single organizational umbrella can easily result in superior outcomes at dramatically less cost than current health care spend.

Amazon has developed a relationship with industry leading Pharmacy Benefits Manager (PBM) Express Scripts, Inc. (ESI), likely to operationalize mail order and facility-based pharmacies. Given ESI’s history of opacity and hall-of-mirrors transactions – approaches that are directly counter to Amazon’s ethos – it’s tempting to imagine that that relationship is a placeholder until Amazon can devise or identify a more value-based model.
Also, a couple weeks ago, Amazon hired Martin Levine, MD, a geriatrician who had run the Seattle clinics for Boston-based Medicare primary care clinic firm Iora Health. This could suggest that Amazon aspires to deliver clinical services, likely through both telehealth and brick- and-mortar facilities.
All this said, we should expect the unexpected. The A/BH/JPM announcement wasn’t rushed, but the result of a carefully thought through, methodical planning exercise. As it has done over and over again – think Prime video; 2 day, free shipping; and the Echo – it is easy to imagine that Amazon could present us with powerful health care innovations that seem perfect intuitive but weren’t previously on anyone’s radar.
What is most fascinating about this announcement is that it appears to pursue the pragmatic urgency of fixing a serious problem that afflicts every business. At the same time, it may represent an effort to subvert and take control health care’s current structure.
So while we may be elated that a candidate health care solution is raising its head, we should be skeptical of stated good intentions. Warren Buffett’s now famous comment that ballooning health care costs are “a hungry tapeworm on the American economy” ring a little hollow when we realize that Berkshire Hathaway owns nearly one-fifth of the dialysis company Da Vita, a model of hungry health industry tapeworms.
Finally, we should not doubt that this project has aspirations far beyond US health care. The corporatization and distortion of health care’s practices is a global problem that will be susceptible to the same solutions of evidence and efficiency everywhere.
All this is promising in the extreme, but there’s also a catch. The US health care industry’s excesses undermine our republic and have become a threat to our national economic security. The solutions that this A/BH/JPM project will leverage could become an antidote to the devils we all know plague our country’s health care system. That said, we should be mindful that, over the long term, our saviors could become equally or more problematic.
Brian Klepper is Principal of Worksite Health Advisors, which connects health care purchasers to high performance health care services.
Categories: Uncategorized









But nowhere do I hear interest in listening to the doctors about their concerns. At the rate we are going, we just won’t have doctors anymore.
Minor minor quibble with Brian’s excellent piece. ACA was passed and signed March 23, 2010 not mid 2009. BY then the stock market was recovering from the early 2009 lows. UNH stock price was around 32, not 26, so at its recent high of about 248 it was only up 8 times not 10!
The challenges include (1) convincing large provider organizations to put significant dollars at risk based on performance / value metrics, (2) defining and measuring quality / value, (3) deciding how to factor patient non-compliance into the quality measurement process, and (4) creating price transparency tools that will allow both patients and referring doctors to identify the most cost-effective high quality providers in real time and steer more of their business to them. All are easy to articulate but not so easy to execute.
Brian, where’s/what’s the incentive for those disciplines to sign on?
“I know, many say patients are too dumb to search for value in this domain…..but the experts said the same thing at the inception of 401k accounts as an alternative to paternalistic defined benefit plans.”
The “many” are right.
https://www.kiplinger.com/article/saving/T001-C000-S002-the-high-cost-of-401-k-fees-how-much-are-you-payin.html
http://billmoyers.com/2013/09/25/how-401ks-rewarded-the-rich-and-turned-the-rest-of-us-into-big-losers/
Bezos: “Your margin is my opportunity”. Health insurers….even the so called non profits….add 12-14% to provider charges. That is way too much.
Also, The Rand Corporation has conducted well designed large sample studies of employer adopted high deductible plans linked to Health Savings Accounts and the results are impressive. Their big study was 2008 (n=800,000) nationwide. Here is a quote from a Health Affairs article in 2012 “If consumer-directed health plans (CDHPs) grew to account for half of employer-sponsored insurance in the U.S., health costs could drop by $57 billion annually—about 4 percent of health care spending for the nonelderly, according to a Rand Corp. study, published in the May 2012 issue of the journal Health Affairs.” The key is for patients to be able to directly benefit financially from prudent use of health care services. I know, many say patients are too dumb to search for value in this domain…..but the experts said the same thing at the inception of 401k accounts as an alternative to paternalistic defined benefit plans.
I agree. In retail, Amazon doesn’t seem to care about making money which makes them especially hard to compete against. Amazon CEO, Jeff Bezos, strikes me as a visionary in the mold of the late Edwin Land who founded Polaroid, the instant camera company. He was once quoted as saying “The factory is an extension of the laboratory.” Polaroid still made a lot of money in its day and was a great stock for a long time but nobody wants to compete against companies that don’t care about at least earning enough to cover their weighted average cost of capital.
Amazon only makes money on its web services. My bet is that they don’t eallyunderstand health care and they won’t accomplish much.
Steve
Will they pay less for drugs, not just a little less but a lot less? Will they pay providers less and control premiums payers lust for squeezing every last breath out of their existence on this planet no matter the cost? Will they be able to turn back hospital consolidation? And if they do all this what will happen to their stock investments in health care industries?
Good article, Brian. Thanks.
I hope you are right!…but we are still stuck with our canonical defect in the sector: third parties are paying for everything.
We need to go to refundable vouchers so that the patient and the providers feel they are, at least in part, paying….while we can still provide the altruism necessary.
I disagree. They’re more likely to bring prices down by streamlining the exorbitant excesses in US health care:choosing clinical and administrative providers who can financially guarantee that they’ll deliver better health outcomes at lower cost than conventional approaches in high value niches like musculoskeletal care, cardiometabolic care, oncology, surgical mgmt, drug mgmt, imaging mgmt, claims review, large case mgmt, large claims resolution and so on. These “high performance” organizations exist but are ignored by the health plans because they drive down total spend and net earnings.
They are just going to bring prices down through large dominant purchasing (monopsony). Read about monopsony before being too enthusiastic. It is not the best way to go economically and it has a dead weight cost to society.
Add them to the long list of people who thought they were going to revolutionize healthcare, only to screw it up even more.
Brian, I think different pieces of the healthcare system need different strategies to address the cost issue.
Two things that hospitals and skilled nursing facilities have in common that drive high costs are that both are labor intensive businesses that must operate every day and around the clock. So, we should be trying to drive as much inpatient hospital care as possible out to hospital outpatient settings and non-hospital owned ambulatory surgical centers, imaging centers, rehab centers, etc. For nursing homes, we need to increase the percentage of residents who execute living wills or advance directives to reduce futile care at the end of life. We also need closer monitoring of physical therapy services which are often done mainly to drive revenue for the home with little or no benefit to the patient. Medicaid needs to stop just mindlessly paying for these services and provide more oversight.
Specific physician services like hip and knee replacements, heart surgery and courses of cancer treatment lend themselves well to reference pricing with some adjustments for higher risk cases. The same applies to imaging which should be priced based mainly on machine time and set-up time irrespective of which part of the body is being examined.
The FDA can speed up its drug approval process and reduce its costs to encourage new generic drug manufacturers to enter the market to provide additional competition when there are only one or two competitors charging very high prices. Expensive specialty drugs lend themselves well to QALY metrics imposed by payers which can also take into account non-drug healthcare costs that patients also require. There needs to be some reasonable limits placed on how much society should be expected to pay to keep one person alive.
Primary care is a relatively small part of total healthcare costs. I’m not a fan of capitation because I think it would lead to doctors seeing far fewer patients per day. I also don’t like physician practices being owned by hospital systems where they get pressured to drive revenue for the mother ship and to keep as much care as possible within the system whether or not it’s in the patient’s best interest.
I also note that the litigiousness of our society as compared to other societies probably drives the medical specialty societies to develop practice patterns that define the standard to care to include more intensive testing and perhaps more frequent checkups vs. practice patterns in other countries. This is where and how most of the defensive medicine occurs in the U.S. in my opinion. It’s not about making money. It’s about avoiding lawsuits and staying out of court.
In a word, our Federal government is on the trail to national bankruptcy on the back of our nation’s excessively expensive healthcare industry. The politicians are fixed on the possibility of a $1 Trillion addition to our national debt in the next 10 years from the recent change in Federal taxation. But, there is no recognition that our nation’s ‘health spending’ will create a $4 Trillion, or more, addition to our national debt during the same 10 years.