
By MATTHEW HOLT
There has been a ton of analysis about COVID-19 and how bad it will get. Some like Joon Yun and Jeremy Faust say the panic is worse than the disease. Others have run the infection rate numbers and predicted that the US will run out of hospital capacity in early May and in Washington state much earlier (end of March).
But there’s no doubt that in the last week or so, sentiment has changed. This week I and 45,000 of my best friends are at home, not at HIMSS in Florida. Many big gatherings like SXSW, Comic-Con and Coachella have been cancelled. Most corporations that can are asking employees to work from home. Just this morning my local school district in California called off school plays and any gatherings with more than 100 people.
Part of this is the inevitable response to the ridiculous posing of Trump. He showed up at the CDC wearing a campaign hat and declared that he was a great doctor to be because his uncle was at MIT. The Director of the CDC and later the Surgeon-General made toadying remarks about how amazing he was. And neither Pence, Azar, Carson or anyone else allegedly in charge can give a straight answer to anything.
The nation has realized that there is no help or even basic honesty coming from the Federal government. This is after the CDC screwed up the creation of basic testing kits which put the US in a situation where it just can not know the extent of the outbreak. China denied the outbreak, then had to put Wuhan and much of their economy on lockdown. Iran may be in worse shape.
Meanwhile South Korea, Singapore and Taiwan have managed their outbreaks with very rapid testing, quarantining of those infected, and extremely rapid response. The US is still blundering around. Now the private sector is trying to step in as the Feds misstep again and again.
But a likely scenario is that many regions in the US will become like Northern Italy.
And the stories coming from there show what happens when the hospital system gets overwhelmed. Here is a thread from an ICU doctor. (I’ve featured a couple of tweets but read the whole thing).
Now we have to imagine that coming here. The big question in my mind is, can the US system organize itself? The US is not China. We’re not going to be able to build new hospitals in a few days. But can we “pull an Italy”?
My huge concern is that we have very different systems. Italy has essentially a UK-style public health service. Organizationally, primary care in the community is run by independent doctors, but anyone needing specialty care is referred to specialists who are based in and work for hospitals. Note that despite having that terrible socialized medicine, Italy has more resources than we do, as ex-Harvard and now Brown Prof Ashish Jha pointed that out when tangling with a right wing idiot.
But think about what that means in Italy. Basically every medical resource and specialist in Italy is already in the hospitals. They already work for one organization. They have already mobilized by turning every available space and operating room into an ICU. And “there are no more surgeons, urologists, orthopedists, we are only doctors who suddenly become part of a single team”. Don’t forget that this single team is already all getting paid by one source and are basically all salaried.

Now think about the US. Hospitals don’t employ most of their doctors. Yes, the bigger ones have hospitalists and residents, and may contract with groups for emergency department doctors, radiologists and the like. But they are organized in a totally different way. Much of the capacity of the US system is in outpatient units such as ambulatory surgery centers and free standing urgent care centers and emergency departments.
Then there is the biggest bugaboo of the American system. Who gets paid how and who does what? Most American physicians are paid directly fee for service or working for an organization that does. They make their living stamping out medical widgets (office visits, surgeries, procedures, reading images), and they in general do it for an organization that is not a hospital. The Italian scenario would require that a huge proportion of physicians and other health professionals are going to have to change on a dime. They are going to have to go suspend their daily activities, go back into hospitals or other temporary centers, treat patients with a disease that they’ve never seen, look after themselves, and their families. And they will need to do all this without knowing how or perhaps whether they will get paid.
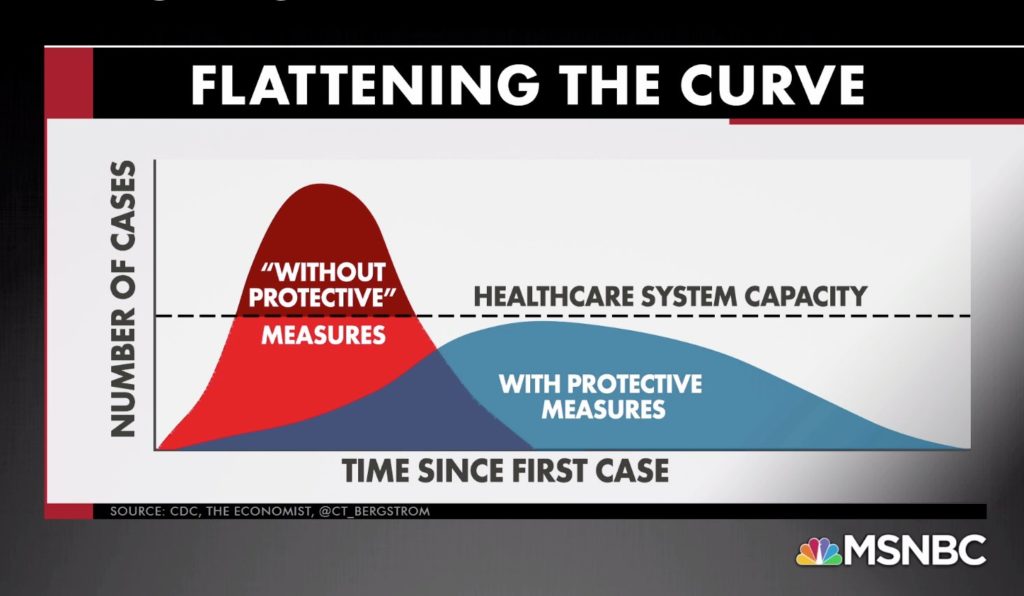
There’s been a lot of chatter about whether we can delay the onslaught of COVID-19 cases to enable hospital capacity to cope, and the “flattening the curve” chart has popped up frequently.
My question is, if we end up in that red zone where Italy is now and need to allocate all our resources in a similar way, who is in charge of the American health care system who can make that happen?
My fear is that the answer is no one.
Matthew Holt is the Publisher of THCB
Categories: Uncategorized









It turns out that according to the most recent data available, Italy has 12.5 ICU beds per 100,000 of population and the U.S. has 34.2. Also, Italy has the 2nd oldest population in the world after Japan. Of those who died so far in Italy from from the Covid 19 virus, 58% were over 80 years old and another 31% were in their 70’s.
Matthew — I read sometime back that compared to the UK, the U.S. has roughly five times more ICU beds per 100,000 people. I wonder if you have or know of comparable data for Italy and the other major Western European countries.
I get no fact based comments at my gym that this is just like the flu (Trump’s hoax theory) in that only the old and vulnerable are at risk. That may be, but everyone is more at risk as there is no vaccine. The homeless and other un/under insured are more at risk as are rural residents with no local hospital with many closed.
Even if the young and healthy are fine, what do they owe the rest of us to help stop the spread and pay for the necessary health care. Would they want their vulnerable relative exposed/infected? What do they owe the health care workers who will need to be well and on the job.
As usual in the U.S. it’s about “me” not “we”.
Matthew never disappoints.
very informational content!
As a health advisor, I would like to suggest people take some precautions while you are in the office or anywhere.
for more i have written my blog here you can check it
I don’t see us “pulling an Italy”. Your analysis is spot on. Nobody has the power or ability to turn American health care into a Covid-19 first responder.