
BY ANISH KOKA
The COVID pandemic was supposed to herald the end of the idea that a smaller government is a better government. The experts who desperately seek to be in charge of a sprawling bureaucratic state told us that it was only a powerful central authority that could do what was needed to safeguard individual liberties at a time when a highly contagious respiratory virus was spreading across the globe.
New Zealand may have imposed draconian policies that did not even allow its own citizens to return, but scenes of cheering unmasked New Zealanders stood in sharp contrast to empty seats in American stadiums when teams were allowed to play. If only US politicians possessed the iron will of New Zealand premier Jacinda Arden, Americans too could have ‘freedom’.

But in so many ways, the New Zealand example demonstrates the utter foolishness and shortsightedness of the central planners that seized control globally. A year after New Zealand took their victory lap COVID arrived in New Zealand and a very much masked Prime Minister noted that “very soon we will all know people who have Covid-19 or we will potentially get it ourselves”

Suddenly it was NewZealanders that were now almost completely vaccinated (with a vaccine developed and tested in America) that were anxious, and the populations hardened by living through the inevitable viral waves that were filling stadiums.
It turned out to be American college football fans, generally not known for their knowledge of statistics, epidemiology or virology that stood up to the tyrants and their hopelessly futile mitigation measures. Covid experts wearing respirators to grocery stores may have been unaware that people sick with COVID in hospitals were rapidly waning in the Fall of 2021, but college football fans somehow sensed it was time to stop listening to the credentialed talking heads and resume pre-pandemic life.
And it was joyous.
Doom and gloom predictions rained down from the expert class as these scenes unfolded in college towns across the nation, but no mass casualty events followed.
The college football fans had it right.
No one could say it definitely at the time, but the padded daily death numbers on dashboards were increasingly irrelevant. For the most part hospitals and health systems never felt anything like what they dealt with in 2020 when the virus first appeared. It was the experts with their covid dashboards, community transmission levels, and their risk calculators that were wrong.
Looking back its easier to see how this all happened. There was little question that the virus that emerged in the spring of 2020 in the United States was a bad virus. Early on, it had a mortality rate that was multiples of the flu virus for almost every age group (even though the absolute risk to the young and healthy was always very low). It was this high relative risk that underpinned many of the calamitous risk avoidance actions undertaken by public health officials.
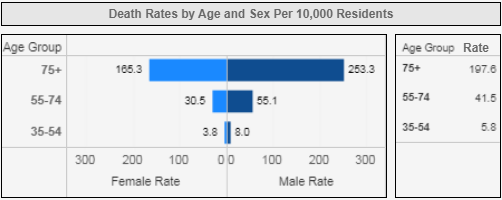
Mortality rate by age and sex due to COVID in Philadelphia (Accessed 4.2021). Source: City of Philadelphia
The problem was that the public health officials became anchored to an early model of risk that they are still struggling to update 2 years later despite the paucity of COVID pneumonia cases in hospitals.
College football fans were unencumbered by covid dashboards and pseudoempiric models. Their risk assessment was based on the local knowledge of who was dying and sick from COVID in their community, and judged that attending a game was a risk worth taking.
Hindsight makes it easy to see that the wheels were never going to stay on for long on the public health response because the experts turned out to be horrendous at critical analysis of data in real-time. The appraisal of the evidence for community masking was a perfect example.
Not suprisingly, real people delivering Ubereats to COVID academics wearing n95 masks while giving zoom interviews to CNN from their basement understood the real world effectiveness of masks better than the talking heads busy informing their echo-chamber of the latest academic paper on community masking.
Masks are certainly easy to mandate, and it is visually powerful and obvious to see scenes of masked 2-year old’s in daycare, but it only takes a few minutes of observation of children, or adults to realize that the general public donning a mask doesn’t function anything like the surgeon in an operating room wearing a mask. I, along with many others in March of 2020 were very early to don masks in and out of the hospital in the hopes the mask was some magic bullet, but the anecdotal evidence and the data on the mass public wearing masks is far from convincing.
Consider the fact that the governor of North Dakota implemented a statewide mask mandate in the Fall as COVID surged. South Dakota did not. Yet in the months that followed, the rise and fall in cases and deaths were almost indistinguishable in the two states.
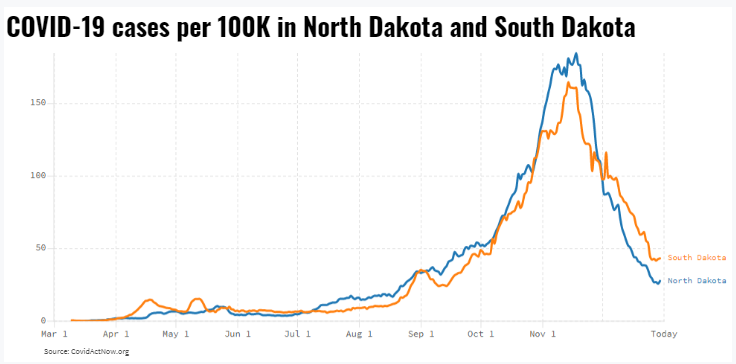
North Dakota implemented a mask mandate in the Fall of 2020 as COVID cases surged, South Dakota did not. No perceptible difference in COVID outbreaks between the states is observed.
It is plausible that the people of South and North Dakota acted in unison regardless of what the Governors’ mansions in their respective states were saying, but even if that were the case, it would still suggest the edicts of governors are irrelevant. (This isn’t just one cherry picked anecdote, Ian Miller authored an entire book full of the futility of mask policies globally)
Beyond the overwhelming amount of real world data, the experts even screwed up the assessment of the two randomized controlled trials on masks that were done during the pandemic. A Danish Randomized Controlled trial that studied how effective mask wearing was early in the course of the pandemic was ignored to the point that authors had difficulty finding anyone from the intelligentsia willing to publish their study because the results didn’t align with public health group-think of the moment. As little Mussolini’s in every major city rushed to implement mandates on masks, this study was delayed for months because elite journals were terrified about publishing a trial that suggested mask wearing in the community didn’t work.
The actual study was pretty simple – 6000 participants in Denmark were randomly assigned to surgical mask wearing or not when outside the home. The masked group had 42 infections, while the control group had 53 infections. The small number of events meant the results were compatible with a 46% reduction in infection, or a 23% increase in infections — far from convincing evidence of the benefits of masks. The study was conducted at a time when most in the community were practicing social isolation but were not generally wearing masks, so critics noted the study could only speak to the type of protection mask wearers may gain when wearing masks while surrounded by others not wearing masks. So, on its own, the study couldn’t rule out the possibility that community-wide masking may mitigate the spread of the virus, just that surgical masks as worn by the general public when interacting with a socially distanced world provide little protection to individuals.
The COVID soothsayers were undeterred, and even worse, took credit for their bold mask leadership when viral waves dissipated. The second waves that came despite mask policies were always because of misbehaving deplorable trump voters, and even when the n95, respirator wearing crowd got COVID, it was some other irresponsible person in some far off place that was clearly to blame.
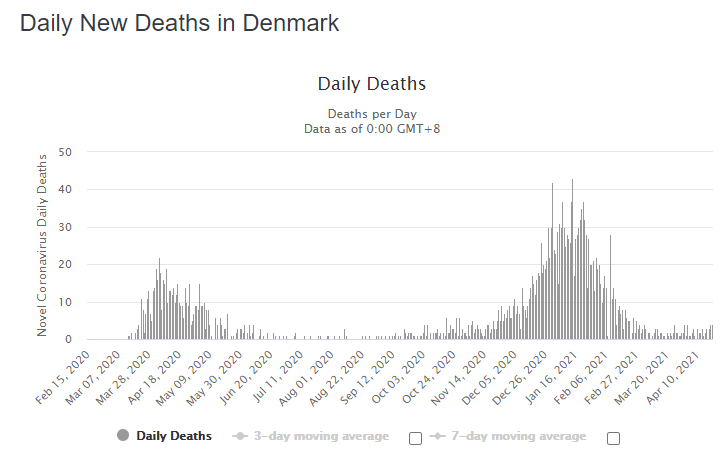
Denmark’s second wave of COVID death came despite masks being ubiquitous
While the Danish trial was ignored, the mask trial that was widely publicized was a massive Bangladeshi randomized control trial that came out with the pleasing conclusion that community masks were effective in stopping COVID.
But if you actually read the results of the trial, it turns out that there was a difference of 20 symptomatic cases over 8 weeks in a population of 340,000 studied.
These results were too fragile to be definitive. Slight imbalances in the two comparator groups could easily invalidate the tiny difference in cases noted. The legacy media, of course, didn’t care to ask the hard questions of the public health intellectuals and politicians that took these weak results as a reason to trample on individual rights in the name of public safety.
The reality was that the science on masks and almost everything else was opinion masquerading as science. The discerning public quickly recognized that scientists making pronouncements about cruise ship travel, masks, or backyard gatherings are just signaling the set of choices they would make informed by their threshold for risk. There is little that was truly empirical about any of this.
It could be that the public health officials who came to some internal consensus on groups gathering and mask mandates based on COVID community positivity rates are a risk-averse group that also shied away from buying houses with swimming pools. There is nothing wrong with these decisions to mitigate personal risk, but they may not be what you choose.
Unfortunately, COVID created a class of people that saw it as their job to decide what was best for you and your family. This group of moral busybodies has always wanted to choose what schools your children should go to, what you should be allowed to eat, what car you should drive, and who you should pray to. COVID was a dream – it gave them control over almost every aspect of American life.

And so, we have the spectacle of 3-year old’s masked and schools closed indefinitely because a group of people far away that don’t know you and are unlikely to share your values are making decisions on what risks you and your children should be allowed to take.
The path traveled over the last two years make abundantly clear the unelected public health bureaucrat class possess neither the competence to understand the uncertainty around the science, or the humility to wield the power that was given to them. And for these sins, they should never again have any control of anything, let alone the keys to the world’s largest economy.
If there is a silver lining in any of this, it’s that the pandemic didn’t strengthen the case for central planners and the nanny state, it destroyed it. Schools didn’t need to be closed for the better part of 18 months, 3 year olds do not benefit from masking continuously, cloth masks may be about as good as preventing COVID as yoga pants, vaccinated people can still acquire and transmit COVID, and shutting down the US economy and printing ten trillion dollars is a very, very bad idea.
Let’s hope everyone has learned a very important lesson. When the next crisis does arrive, don’t ask the experts what to do.
Talk to college football fans.
Anish Koka is a cardiologist. Follow him on twitter @anish_koka.
Categories: Uncategorized









This is pretty sorry stuff from someone who claims to be a physician. There is pretty good data that masks work, but they arent a force field, they just reduce risk. The longer you are exposed the less well they work. (Less true for PAPRs and N 95s.)
Since you apparently believe that the only reason people in public health formulated policies was to control, how did you phrase it? “choose what schools your children should go to, what you should be allowed to eat, what car you should drive, and who you should pray to” why are you even posting on a site devoted to medical issues. I am sure there are any number of political blogs that would accept you. I would strongly suggest from the tenor of your writing that you look for those who espouse conspiracy theories and you should be right at home. Very clear you dont want any discussion, just an opportunity to rant.